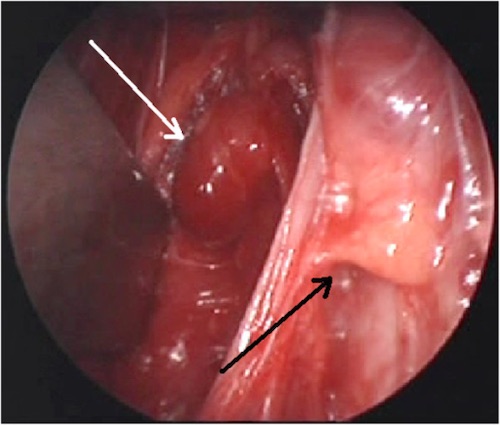
Parathyroid Adenoma (White Arrow) and Normal Parathyroid (Black Arrow) 1
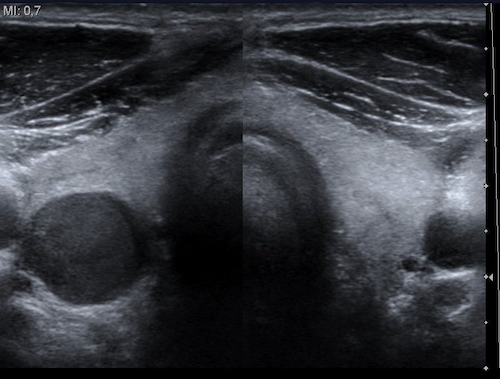
Parathyroid Adenoma on US 2

Parathyroid Adenoma on Sestamibi Scan 3
Parathyroid Adenoma (White Arrow) and Normal Parathyroid (Black Arrow) 1
Parathyroid Adenoma on US 2
Parathyroid Adenoma on Sestamibi Scan 3