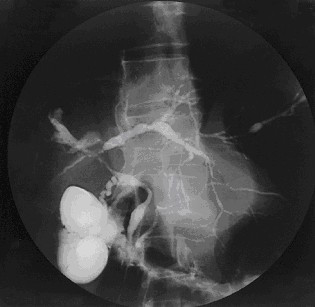
Biliary Tract: Primary Sclerosing Cholangitis (PSC) Primary Sclerosing Cholangitis (PSC) BasicsChronic Autoimmune Fibrosis of the Biliary TractAffects Intrahepatic Bile Ducts (15%), Extrahepatic Bile Ducts (10%) or Both (75%)May See Multiple Strictures Throughout the Entire Biliary TreeMost Common in MenStrongly Associated with IBD (Especially Ulcerative Colitis)Prevalence: 60-90%No Improvement After Colon ResectionHigh Risk of Cholangiocarcinoma (10-20%)PresentationCauses Biliary Stricture with Chronic Cholestasis & Eventual CirrhosisCommonly ASx at DiagnosisSx: Fatigue, Pruritis, Abdominal Pain & JaundiceMay Show Signs of Decompensated Liver Failure if Presenting LateDiagnosisDx: MRCP/ERCP (“Beaded” Bile Ducts)Labs:Elevated LFT’s; Particularly Alkaline PhosphataseAtypical P-ANCA (Perinuclear Antineutrophil Cytoplasmic Antibody)Always Check CA 19-9 for CAAlways Check IgG4Immediate Colonoscopy on Dx to Evaluate for IBDTreatmentTemporary/Sx Relief:Ursodeoxycholic Acid (UDCA)If Dominant Extrahepatic Strictures: Consider ERCP & StentOther Potential Medical Options: Cyclosporine, Methotrexate, Azathioprine or ABXAvoid:Generally Avoid Choledochojejunostomy as TXP is PreferredNo Benefit: Cholestyramine or ColchicineDefinitive Tx: Liver TXPCancer Screening After DiagnosisAbdominal US or MRI/MRCP Every 6-12 MonthsCA 19-9 Every 1 YearColonoscopy at Diagnosis & Every 1-2 Years PSC with “Beaded” Bile Ducts on MRCP 1 IgG4-Associated Cholangitis BasicsMost Frequent Extra-Pancreatic Manifestation of Autoimmune PancreatitisRarely Occurs in Absence of PancreatitisPossibly Manifestation of Same Disease as PSCTreatmentTx: Steroids References Worthington J, Chapman R. Primary sclerosing cholangitis. Orphanet J Rare Dis. 2006 Oct 24;1:41. (License: CC BY-2.0)