Tachypnea Leads to Hypocapnia & Respiratory Alkalosis
Presentation
Many are Asymptomatic
Dyspnea – Most Common Symptom
Pleuritic Chest Pain
Cough
Wheezing
Hemoptysis
Tachypnea
Tachycardia
Fever
Symptoms of DVT
Wells Score
Predicts Probability of PE
Factors:
Physical Findings of DVT – 3 Points
No Better Alternative Diagnosis – 3 Points
Tachycardia (HR > 100) – 1.5 Points
Immobilization (≥ 3 Days) or Recent Surgery (< 4 Weeks) – 1.5 Points
History of DVT/PE – 1.5 Points
Hemoptysis – 1 Point
Malignancy – 1 Point
“Traditional” Wells Interpretation:
> 6: High Probability
2-5: Moderate Probability
0-1: Low Probability
“Modified” Wells Interpretation:
> 4: PE Likely
≤ 4: PE Unlikely
Diagnosis
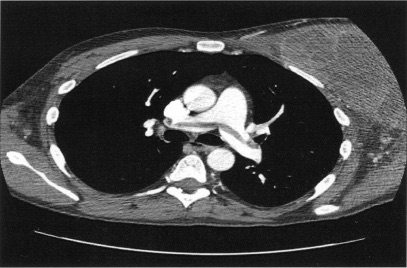
Dx: CT Pulmonary Angiogram (Gold Standard)
If Inconclusive or Not Available Consider Ventilation-Perfusion Scan
Low-Moderate Probability: Consider D-Dimer First
PE Likely Excluded if D-Dimer < 500 ng/mL & Would Not Need CT
If Unstable & High Clinical Probability: Empirically Treat Before Definitive Diagnosis
ABG Findings:
Hypoxemia
Respiratory Alkalosis
Widened Alveolar-Arterial Oxygen Gradient
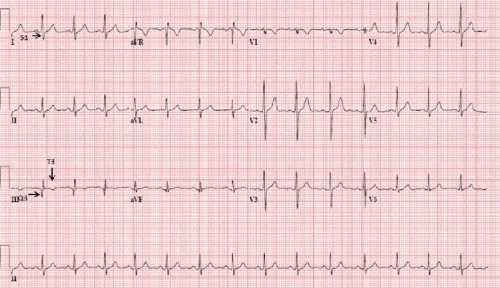
Classic ECG Findings:
Tachycardia – Most Common EKG Finding
S1Q3T3 Pattern (Indicates Right Ventricle Strain) – Rarely Seen
T1-4 Inversion
Echo Findings:
Left Ventricle – Small but Normal Systolic Function
Septal Flattening (RV Pressure Overload)
Right Ventricle – Severely Dilated with Reduced Systolic Function/Wall Hypokinesis
Pulmonary Artery Hypertension
McConnell Sign – RV Dysfunction with Akinesia of Mid-Free Wall but Normal Motion at the Apex
D-Sign – Left Ventricle is “D” Shaped Due to Flattening of the Interventricular Septum from Right Ventricular Overload
D-Dimer Highly Sensitive but Not Specific
Treatment
Stable: Anticoagulation
Unstable & High Probability: Systemic Thrombolytics
If Contraindicated: Embolectomy (Surgical or Endovascular)
Saddle Pulmonary Embolism 1
S1Q3T3 on EKG 2
References
Daher IN, Bathina JD, Bukhari FJ, Yusuf SW. Saddle pulmonary embolism with normal right ventricular function: a treatment enigma. JRSM Short Rep. 2010 Jun 30;1(1):12. (License: CC BY-NC-2.0)
Arshad H, Khan RR, Khaja M. Case Report of S1Q3T3 Electrocardiographic Abnormality in a Pregnant Asthmatic Patient During Acute Bronchospasm. Am J Case Rep. 2017 Feb 1;18:110-113. (License: CC BY-NC-ND-4.0)