Pulmonary Physiology
- Develops From 7 Months Gestation to 10 Years Old
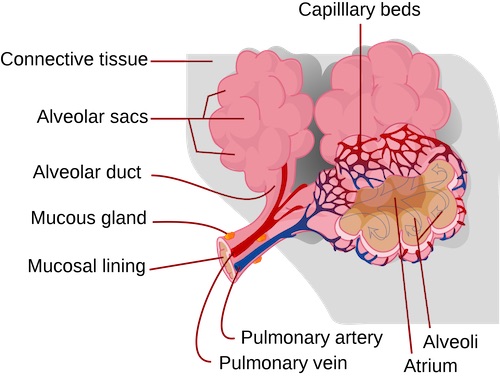
- Pneumocytes
- Type I: Gas Exchange
- Type II: Produce Phosphatidylcholine/Surfactant
- Lowers Surface Tension & Keeps Alveoli Open
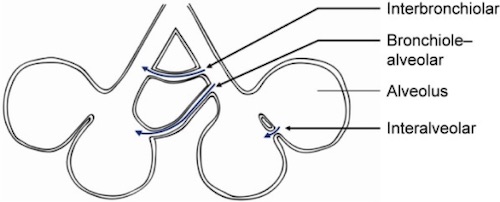
- Collateral Ventilation:
- Pores of Kohn: Direct Air Exchange Between Alveoli
- Channels of Lambert: Air Exchange from Bronchiole to Alveolus
- Channels of Martin: Air Exchange Between Bronchioles
- Partial Pressure of Oxygen
- Highest Point: Pulmonary Capillaries
- Slightly Less by the Time Blood Reaches the Atrium
- Lowest Point: Coronary Veins
Ventilation/Perfusion
- Dead Space: Area Ventilated but Not Perfused
- Causes Increased PCO2
- Most Common Cause: Excessive PEEP (Induces Capillary Compression)
- Shunt: Area Perfused but Not Ventilated
- Causes Decreased PO2
- Most Common Cause: Atelectasis
Ventilation/Perfusion (V/Q) Ratio
- Causes of High V/Q Ratios:
- Dead Space
- Normal Lung Apex
- COPD
- Pulmonary Embolism
- Causes of Low V/Q Ratios:
- Shunting
- Normal Lung Base
- Asthma
- Pulmonary Edema
- Ratio Changes with Body Positioning