Diagnosis
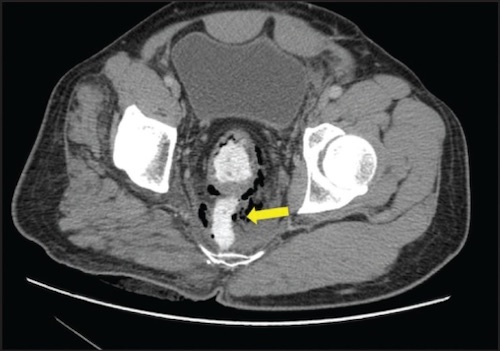
- Start with a CT Using Triple-Contrast (Oral, IV & Rectal)
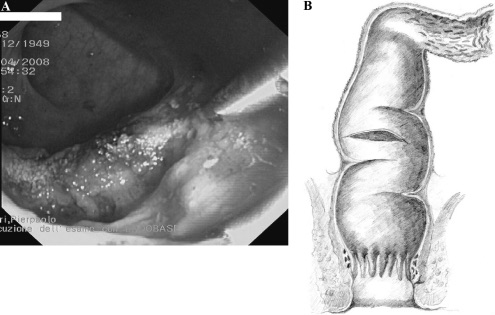
- All Suspected Should Undergo Rigid Proctoscopy
- *May Miss Extraperitoneal Injuries without Endoscopy
Treatment of Intraperitoneal Injuries
- Treated Similar to Bowel
- Non-Destructive: Primary Repair
- Destructive: Resection – LAR
- Diverting Ileostomy if Low (High Risk for Leak)
Treatment of Extraperitoneal Injuries
- High: Same as Intraperitoneal
- Low-Middle: Primary Repair (If Able) & Diverting Colostomy
- Repair Attempted through a Transanal Approach
- Loop Sigmoid Colostomy Generally Preferred – Consider End Colostomy for Devastating Injuries
- Can Take Down in 6-8 Weeks
- Historical Considerations:
- *Presacral Drainage (Previously Recommended for Extraperitoneal Injuries) is Inadequate & Should Not Be Pursued
- *Distal Rectal Washout is Outdated & May Actually Increase the Risk of Infectious Complications