Type I – Small, Confined to Rectus, Does Not Cross Midline
Type II – Confined to Rectus, Crosses Midline
Dissects Along Transversalis Fascial Plane
Type III – Large, Not Confined
Usually Below Arcuate Line (Severe Bleeding – No Aponeurosis to Contain)
Often See Blood in Prevesical Space of Retzius
Diagnosis
Dx: CT or US
Treatment
Stable: Observation
Unstable or Enlarging: IR Angioembolization
Surgery
Procedure: Surgical Evacuation & Vessel Ligation
Indications:
Skin Necrosis
Unstable or Enlarging with Failure of Angioembolization
Incision: Midline or Paramedian to Expose the Posterior Sheath (Avoid Entering the Peritoneum)
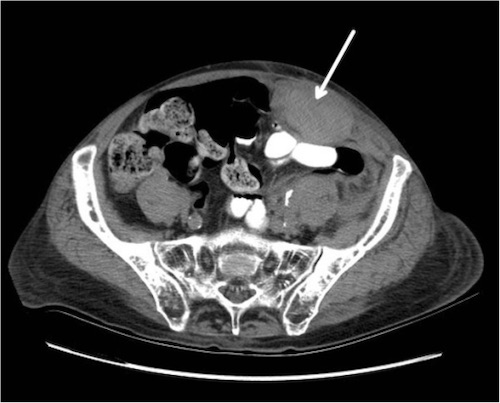
Rectus Sheath Hematoma on CT 1
Mnemonics
Types of Rectus Sheath Hematomas
Type 1: 1 Side
Type 2: 2 Sides
Type 3: Past the Two Sides
References
Sullivan LE, Wortham DC, Litton KM. Rectus sheath hematoma with low molecular weight heparin administration: a case series. BMC Res Notes. 2014 Sep 1;7:586. (License: CC BY-2.0)