Renin-Dependent, Euvolemic Hypertension – Renin Produced by Affected Kidney
Bilateral Disease: No Compensatory Response
Volume-Dependent, Hypervolemic Hypertension – By Negative Feedback Has Normal/Low Renin
Ischemic Nephropathy
Contralateral Kidney Can Be Injured from Compensatory Systemic Hypertension by RAAS Activation
Generally Only from Severe Disease
Renal Insufficiency With Only Mild-Moderate Hypertension is Unlikely to Improve with Revascularization
Causes
Atherosclerosis
Most Common Cause (80-90%)
Typically Most Severe at the Ostia
Most Common Side: Left
Most Common in Men
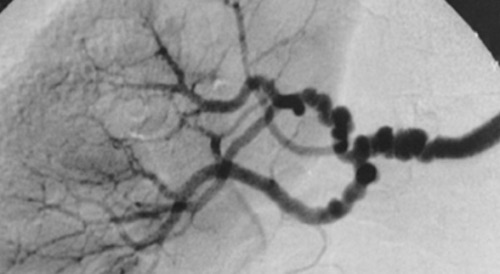
Fibromuscular Dysplasia
Nonatheromatous Noninflammatory Proliferative Process
Most Common in Women Age 20-60
Seen Predominantly in the Middle Segment of the Renal Artery
Typically Affects the Main Artery & Distal Branches
Most Common Site: Right
“String of Beads” Appearance from Alternating Stenosis & Dilation
Other Sites:
*See Vascular: Arteriopathies
Dissection
Aneurysms
Trauma
Diagnosis
Screen: Duplex US
Renal Artery Systolic Velocity > 180 cm/s
Renal Artery-to-Aorta Velocity Ratio > 3.5
CTA or MRA are Excellent Tests but May Risk Nephrotoxicity
Gold Standard: Digital Subtraction Angiography (DSA)
More Difficult & Invasive – Typically Only Used if Planning Reconstruction
Renal Artery Stenosis 1
FMD of Renal Artery, “String of Pearls” Appearance 2
Treatment
Mild-Moderate Disease: Medical Management
Antihypertensives
First-Line: ACE-I & ARB
Often Requires Multiple Medications with Different Classes
In Atherosclerosis Include: Statins & Antiplatelets
Severe Refractory Disease that Fail Medical Management:
Atherosclerosis: Angioplasty with Stent
Fibromuscular Dysplasia: Angioplasty without Stent
If Kidney Atrophic < 6 cm: Consider Nephrectomy
Predictors of Hypertension Improvement After Renal Revascularization
Short Duration of Hypertension Prior to Diagnosis – Strongest Clinical Predictor
Failure of Medical Therapy
Intolerance of Medical Therapy
Recurrent Flash Pulmonary Edema
Refractory Heart Failure
Renal Artery Aneurysm
Basics
Most Common Cause: Atherosclerosis & Congenital Defects
Typically Involves Branch Arteries
Rarely Limited to the Main Artery
Treatment Indications
Rupture
Symptomatic
> 2-3 cm
Pregnancy (High Risk of Rupture/Mortality)
Severe Refractory Hypertension that Fails Medical Management
Treatment
Rupture: Resection & Nephrectomy
May Consider Reconstruction if Stable with Bleeding Quickly Controlled & Straight-Forward Repair
Elective Repair:
Endovascular Stent
Preferred if Limited to the Main Artery
Avoid if Aneurysm Extends into the Branches
Coil Embolization
Open Aneurysmorrhaphy with Patch Angioplasty
Renal Artery Aneurysm 3
References
Chain S, Luciardi H, Feldman G, Berman S, Herrera RN, Ochoa J, Muntaner J, Escudero EM, Ronderos R. Diagnostic role of new Doppler index in assessment of renal artery stenosis. Cardiovasc Ultrasound. 2006 Jan 25;4:4. (License: CC BY-2.0)
Plouin PF, Perdu J, La Batide-Alanore A, Boutouyrie P, Gimenez-Roqueplo AP, Jeunemaitre X. Fibromuscular dysplasia. Orphanet J Rare Dis. 2007 Jun 7;2:28. (License: CC BY-2.0)
Cooper SS, Baldwin R, Mlynarczyk C, Hellenthal NJ. Renal Ganglioneuroma Presenting as an Apparent Renal Artery Aneurysm. Urol Case Rep. 2015 Mar 14;3(3):86-8. (License: CC BY-NC-ND-4.0)