Definitions
- Restorative Proctocolectomy – Complete Colon & Rectum Resection Sparing the Anus for Reconstruction
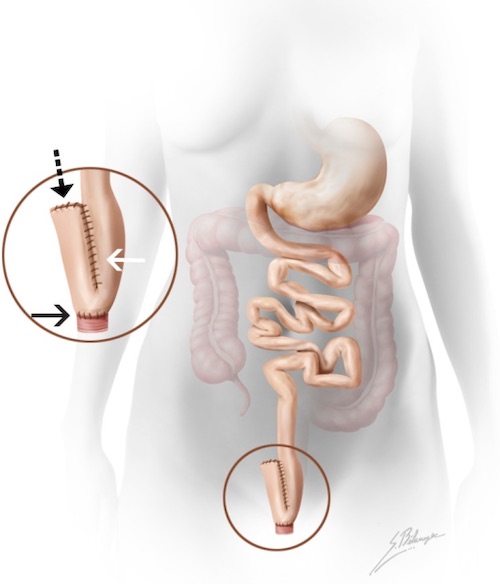
- Ileal Pouch-Anal Anastomosis – Ileum Loop Folded onto Itself Creating a Pouch for Anastomosis
- Pouch Allows Reservoir to Decrease Bowel Movement Frequency
- Often Done as a Two-Stage Procedure with Initial Diverting Loop Ileostomy
Possible Candidates
- Inflammatory Bowel Disease without Rectal Involvement Refractory to Medical Management
- Generally Used in Ulcerative Colitis but Not for Crohn’s Disease
- Familial Adenomatous Polyposis (FAP)
- Severe Colonic Inertia Refractory to Medical Therapy (Ileorectal Anastomosis Preferred)
Contraindications
- Absolute:
- Severe Fecal Incontinence
- Low Rectal CA Involving Sphincters
- Perianal Crohn’s Disease
- Relative:
- Morbid Obesity
- Low Rectal CA with Neoadjuvant Tx
- Non-Perianal Crohn’s Disease
- Prior Extensive Small Bowel Resection
Ileal Pouch Types
- J-Pouch (2-Limbs)
- Preferred Type
- Length: 15-20 cm
- Rare Alternative Types:
- S-Pouch (3-Limbs)
- W-Pouch (4-Limbs)
Techniques to Decrease Tension or Ensure Reach
- Division of Ileum Flush with Cecum
- Complete Mobilization of Small Intestine to the Third Portion of Duodenum
- Full Adhesiolysis
- Transverse-Stepladder Relaxing Incisions Over the Mesentery Under Tension Along SMA Vessels
Pouchitis
- Most Common Long-Term Complication (23-59%)
- Higher-Risk if Resection Due to Ulcerative Colitis
- Infectious Pouchitis
- Cause: Inflammation of Pouch from Infection
- Postoperative Microbiome of Pouch Transitions from Ileum-Like to Colon-Like
- No Specific Pathogens Have Been Consistently Implicated
- Sx: Diarrhea, Bloody Stools, Pain & Fever
- Tx: Oral ABX (Ciprofloxacin #1, Metronidazole or Tinidazole)
- Consider Biopsy to Rule Out Chron’s Disease
- Diversion/Disuse Pouchitis
- *See Large Intestine: Diversion Colitis
- Cause: Inflammation of Pouch from Diversion by Loop Ileostomy Due to Deficiency of SCFA’s
- Preferred Tx: Surgical Reanastomosis
- If Unable to Reanastomose: SCFA Enema
- Consider Topical Anti-Inflammatory (5-ASA/Steroids)