No Prolapse Present: Proctectomy or Fecal Diversion
SRUS Errythema 1
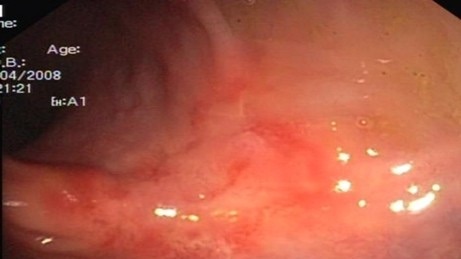
SRUS Ulcer 2
References
Abid S, Khawaja A, Bhimani SA, Ahmad Z, Hamid S, Jafri W. The clinical, endoscopic and histological spectrum of the solitary rectal ulcer syndrome: a single-center experience of 116 cases. BMC Gastroenterol. 2012 Jun 14;12:72. (License: CC BY-2.0)
Katsanos KH, Sigounas DE, Christodoulou DK, Tsianos EV. Isolated rectal ulcer. Ann Gastroenterol. 2011;24(2):121. (License: CC BY-NC-SA-3.0)