COPD/Emphysema – Most Common Cause of SSP (50-70%)
Risk Correlates to Severity of Disease
Interstitial Lung Disease
Malignancy
Tuberculosis (TB)
Sarcoidosis
Cystic Fibrosis
Catamenial Pneumothorax
Pneumothorax Associated with Menstruation
Due to Thoracic Endometriosis
Necrotizing Pneumonia
Diagnosis
Initial Imaging: Chest X-Ray (CXR)
Size:
Small: ≤ 3 cm at Apex or ≤ 2 cm at Hilum
Large: > 3 cm at Apex or > 2 cm at Hilum
Treatment
Stable:
Small: Observation with Supplemental Oxygen
Resolves at 1% Per Day without Treatment
Supplemental Oxygen: 6 L/Minute for 6 Hours
Increases Rate of Reabsorption Up to Six-Fold
Avoid Positive Pressure – Risk for Worsening
Large: Catheter Aspiration or Chest Tube
*Some Propose Conservative Management Even for Moderate-Large Size PTX if Asymptomatic (Debated)
Unstable: Chest Tube
Smaller Diameter (≤ 14 Fr) Generally Preferred
Generally Placed to Water-Seal Initially
Consider Adding Suction (-10 to -20 cm H2O) if Fails
Consider Needle Thoracostomy if Chest Tube Placement Will Cause Delay
Complications
Persistent Air Leak
Air Leak > 4-5 Days
Cerfolio Classification:
Grade 1 (FE): During Forced Expiration Only (Cough)
Grade 2 (E): Only During Expiration
Grade 3 (I): Only During Inspiration
Grade 4 (C): Continuous During Both Inspiration & Expiration
Treatment: Surgery (VATS Thoracoscopy, Resection & Mechanical Pleurodesis)
If No Blebs are Seen – Still Preform an Apical Resection
Recurrent Pneumothorax
Risk: 50-60%
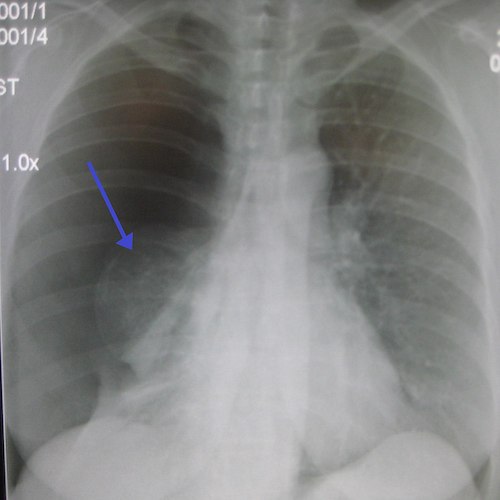
Tension Pneumothorax
Pneumothorax on CXR 1
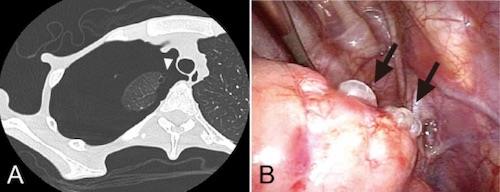
Tension PTX on CT
Pulmonary Blebs; (A) CT, (B) VATS 2
References
Heilman J. Wikimedia Commons. (License: CC BY-3.0)
Ozawa Y, Ichimura H, Sakai M. Reexpansion pulmonary edema after surgery for spontaneous pneumothorax in a patient with anorexia nervosa. Ann Med Surg (Lond). 2016 Mar 3;7:20-3.(License: CC BY-NC-ND-4.0)