Do Not Biopsy – Risk for Tumor Seeding to Scrotal Sac & Metastatic Spread to Inguinal Nodes
Serum Tumor Markers
Seminoma: Beta-HCG & LDH May Be High
AFP Not Elevated
Nonseminomatous Germ Cell Tumors: AFP, Beta-HCG & LDH May Be High
Stromal Tumors: Negative Tumor Markers
May See Elevation of Hormonal Markers
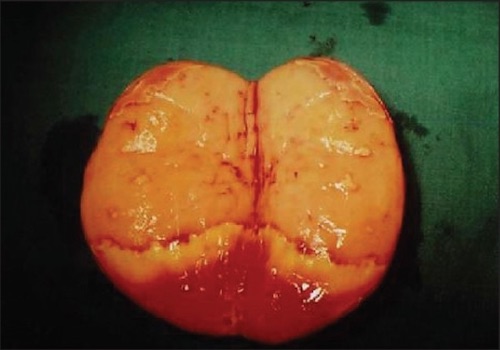
Seminoma, Testicle Opened After Resection 1
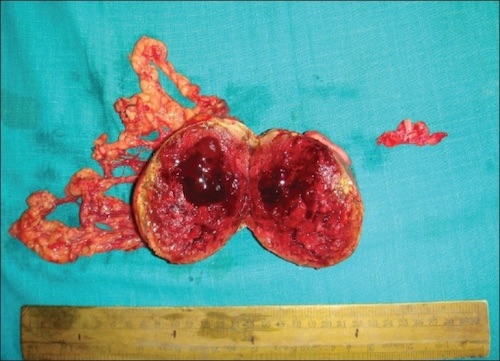
Embryonal Carcinoma, Testicle Opened After Resection 2
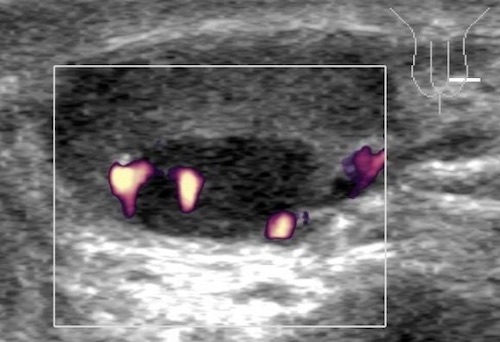
Seminoma US 3
TNM Staging – AJCC 8
TNM
T
N
M
I
Confined to Testicle
1-5 LN ≤ 2 cm
Mets+
II
Invaded Blood Vessels, Lymphatics, Epididymis, Fatty Tissue or Tunica Vaginalis
> 5 LN or 2-5 cm
III
Invaded the Spermatic Cord
LN > 5 cm
IV
Invaded the Scrotum
Stage
T
N
M
I
Any T
N0
M0
II
Any T
N1
M0
III
Any T
Any N
M1
Staging Subgroups Include Serum Tumor Markers (S) – LDH, Beta-HCG & AFP
Treatment
Primary Treatment: Radical Orchiectomy by Inguinal Incision
Inguinal Incision Avoids the Lymphatics of a Scrotal Approach
May Consider Partial Orchiectomy if Polar Mass ≤ 2 cm & Abnormal or Absent Contralateral Testicle
Retroperitoneal Lymph Node Management:
Seminoma: Radiation Therapy
Nonseminomatous or Stromal Tumor: Retroperitoneal Lymph Node Dissection (RPLND)
*Consider Active Surveillance Alone for Stage I with Low Risk for Recurrence
Advanced Disease: Chemotherapy
Radical Orchiectomy – Procedure
Inguinal Incision & Incise External Oblique Fascia (Similar to Inguinal Hernia)
Mobilize Cord (Preserve Ilioinguinal Nerve)
Divide External Spermatic Fascia & Cremasteric Fibers
Deliver Testicle by Gentle Cephalad Traction
Mobilize Cord to Level of Internal Ring
Individually Dissect, Ligate & Divide the Vas Deferens & Gonadal Vessels
High-Ligation at Level of Internal Inguinal Ring (Key Step)
Closure
References
Agrawal S, Bajpai R, Agrawal RK, Gupta TC. Bilateral synchronous seminoma with bilateral cryptorchidism of the testis. Indian J Urol. 2010 Oct;26(4):587-9. (License: CC BY-NC-SA-3.0)
Barmon D, Kataki AC, Sharma JD, Hafizur R. Embryonal carcinoma in androgen insensitivity syndrome. Indian J Med Paediatr Oncol. 2011 Apr;32(2):105-8. (License: CC BY-NC-SA-3.0)
Dieckmann KP, Anheuser P, Sattler F, Von Kügelgen T, Matthies C, Ruf C. Sequential bilateral testicular tumours presenting with intervals of 20 years and more. BMC Urol. 2013 Dec 9;13:71. (License: CC BY-2.0)