Thyroid Nodules
- High-Prevalence in General Population: 37-57%
- Majority (90%) are Benign
- Carcinoma Risk Factors:
- Age Extremes (Pediatrics & Elderly)
- Male Sex
- History of Radiation to Head & Neck
- Most Likely Papillary if From a History of XRT
- Solitary Nodule (vs Multinodular)
- Large ≥ 2 cm
Initial Management
- Initial Testing: Thyroid Function Tests (TFTs) & Ultrasound (US)
- If Patient Is Hyperthyroid May First Consider Scintigraphy (Radioiodine Uptake Scan)
- Hot Nodule/Hyperfunctioning: Benign – No Further Testing
- Cold Nodule: Risk for Malignancy – Further Testing/US is Indicated
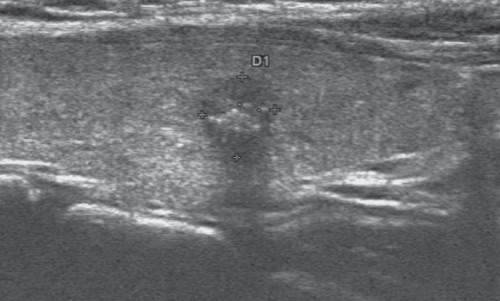
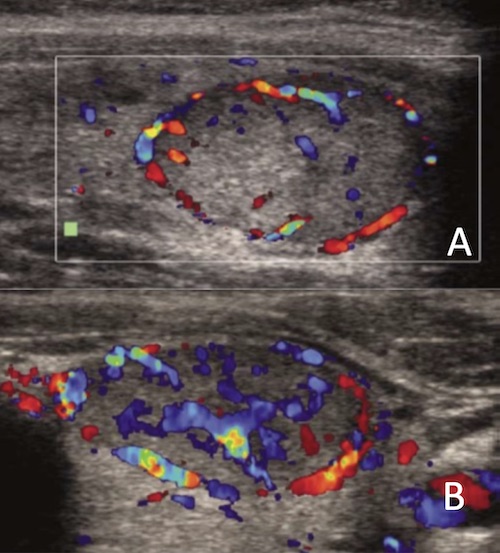
Ultrasound (US) – Concerning Features
- Most Specific:
- Taller > Wide (Normal Grows Radially)
- Microcalcifications
- Heterogenous
- Hypoechoic
- Solid (vs Cystic)
- Lobulated/Irregular Margins
- Hypervascular
Indications for Fine Needle Aspiration/FNA (Based on US)
- Intermediate-High Suspicion: ≥ 1.0 cm
- Low Suspicion: ≥ 1.5 cm
- Very-Low Suspicion: ≥ 2.0 cm
- Purely Cystic: FNA Not Indicated
Bethesda System for Reporting Thyroid Cytopathology (Based on FNA)
- Category I: Nondiagnostic or Unsatisfactory
- Category II: Benign
- Category III: Undetermined Significance
- Atypia of Undetermined Significance (AUS)
- Follicular Lesion of Undetermined Significance (FLUS)
- Category IV: Follicular Neoplasm or Suspicious for a Follicular Neoplasm
- Category V: Suspicious for Malignancy
- Category VI: Malignant