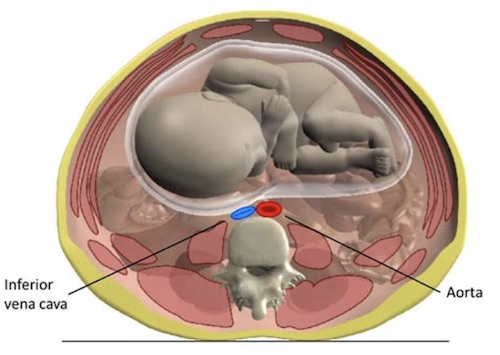
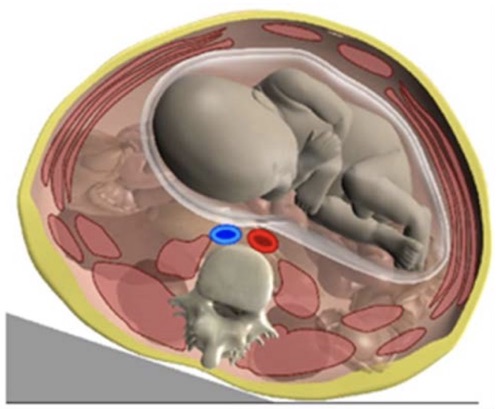
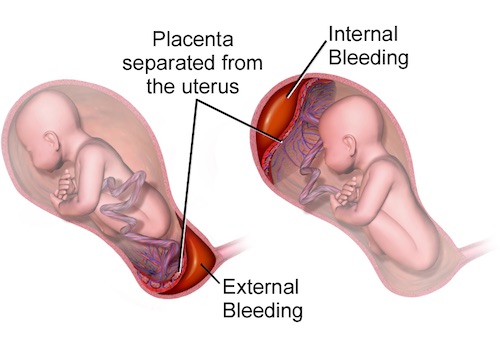
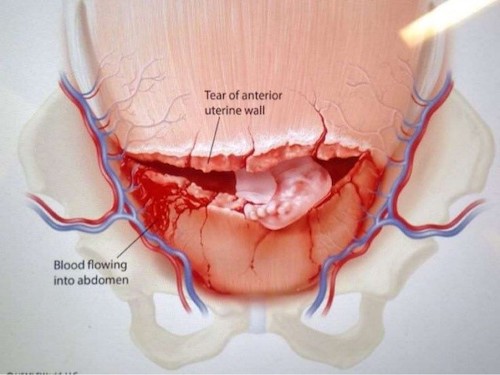
Trauma: Trauma in Pregnancy Pregnancy General ConsiderationsAlways Mother Before BabyMost Common Cause of Death: Intimate Partner ViolenceBlunt TraumaFetal Injury After Blunt Trauma is Rare (< 1%)Most Common Cause of Fetal Death in Blunt Trauma: Maternal DeathPenetrating TraumaHigh Fetal Death Rate – GSW 71% & Stabs 42%Gravid Uterus Provides Protection for Mother with Decreased MortalityFetal MaturityFundal Height (Umbilicus = 20 cm = 20 Weeks)Signs of Maturity:Lecithin:Sphingomyelin (LS) Ratio > 2:1Phosphatidylcholine in Amniotic FluidRadiologyDo Not Delay or Withhold if IndicatedNo Increased Risk of Fetal Defects/Loss if < 5 RadFetus Exposed to About 30% of Maternal Radiation DoseApproximate Fetal Dose:CXR: < 0.001 RadAbdominal XR: 0.1 RadHead CT: < 0.05 RadChest CT: < 0.1 RadAbdominal CT: 2.6 RadTiming:Most Vulnerable During Organogenesis (Weeks 2-8)Generally Safe Past 20 WeeksFAST USAny Amount of Free Fluid is Considered PositivePhysiologic Free Fluid is Small (7-21 cc) & Not Large Enough to Be Seen on FASTManagementsCardiotrophic Fetal Monitoring for ≥ 6 Hours if Over 20 Weeks GestationGive Supplemental O2 in All Pregnant Patients Regardless of SaO2Physiologic Respiratory Alkalosis with Concern for HypoxiaGive Rh Immunoglobulin to All Rh-Negative PatientsGive within 72 Hours of InjuryShould Also Be Given within 72 Hours of DeliveryAortocaval Compression Syndrome (Supine Hypotensive Syndrome)Gravid Uterus Compresses Aorta & IVC When Laying SupinePresentation: Maternal HypotensionTx: Roll to Left Side (Improves Venous Return)If Unable to Adequately Expose Injury Due to Enlarged Uterus: Cesarean Section Aortocaval Compression Syndrome 1 Left Lateral Tilt – Relieves Compression Off IVC 1 Specific TraumaPlacental AbruptionSeparation of Placenta from UterusCauses:Uteroplacental Ischemia from Shock – Most CommonMechanical ForcePresentation: Abdominal Pain, Vaginal Bleeding, Shock or DICKleihauer-Betke Test: Detects Occult Placental HemorrhageUterine RuptureMost Common Site: Posterior FundusMost Common Risk Factor: Previous C-Section Placental Abruption 2 Uterine Rupture 3 Perimortem Cesarean SectionDefinition: C-Section Delivery After Maternal DeathBaby Must Be > 24 WeeksArrest Timing:Best if < 4 Minutes of ArrestContraindicated > 20 Minutes References Queensland Clinical Guidelines. Trauma in pregnancy clinical guideline education presentation E19.31-1-V2-R24. Queensland Health. 2019. (License: CC BY-NC-ND-4.0)Blaus B. Wikimedia Commons. (License: CC BY-3.0)Khcnrc01. Wikimedia Commons. (License: CC BY-SA-4.0)