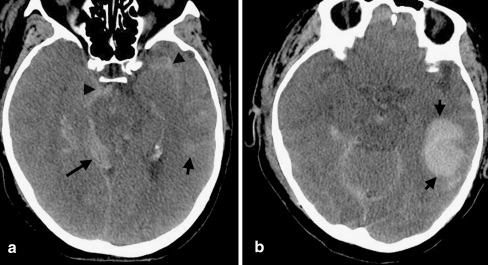
Cerebral Contusion (Parenchymal/Hemorrhagic Contusion)
- Bruising of the Brain from Multiple Punctate Hemorrhages
- May See Surrounding Edema & Necrosis
- Most Remain Small & Surgically Insignificant
- Evolve Over Time – May Worsen or Not Even Be Evident on Initial CT
- Often See “Coup & Countercoup” Injuries
- “Coup” – Injury at the Site of Head Impact
- “Countercoup” – Injury Remote from the Site of Head Impact (Classically Directly Opposite)
- Most Common Sites: Frontal Base and Anterior Temporal Lobes