AAST Abdominal Vascular Injury Scale
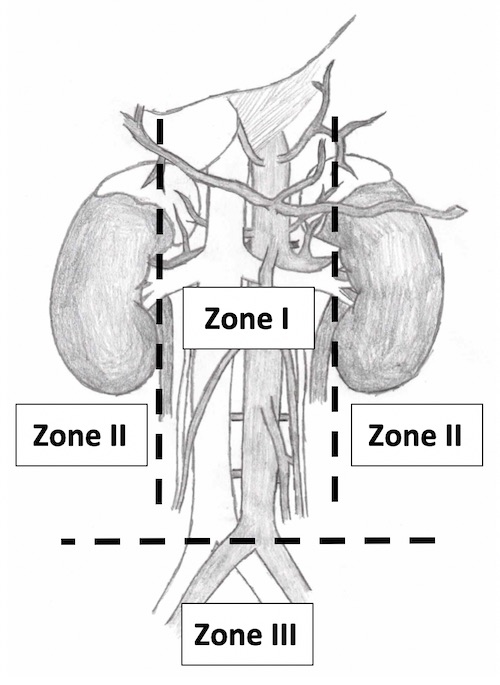
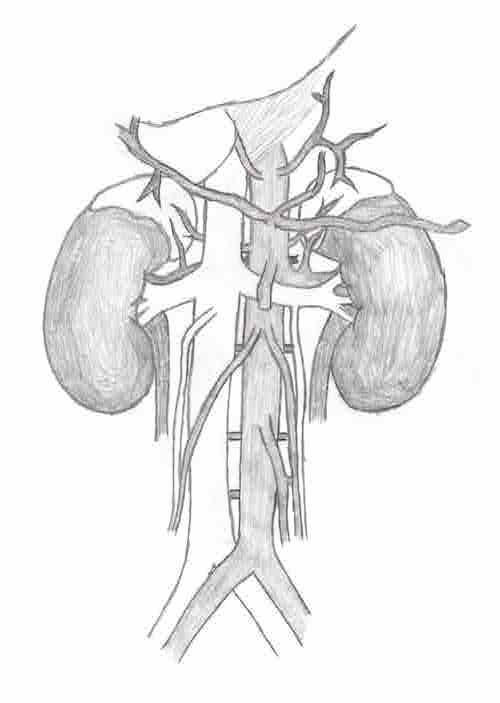
Retroperitoneal Hematoma Management
- Zone I (Central): Mandatory Exploration
- *Between Kidneys from Diaphragm to IVC Bifurcation
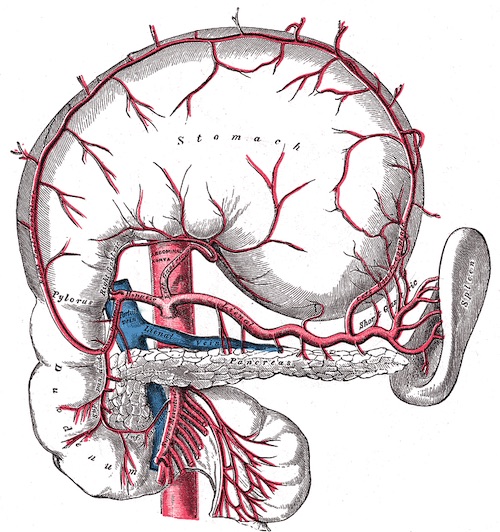
- Associated with Pancreaticoduodenal & Major Vascular Injury
- Zone II (Lateral):
- Penetrating: Selective Exploration
- Blunt: Open Only if Expanding, Pulsatile or with Active Hemorrhage
- *First Step: Palpate Contralateral Kidney to Assess Size & Determine Need for Heroic Measures to Save Ipsilateral Kidney
- Zone III (Pelvis):
- Penetrating: Mandatory Exploration
- Blunt: Open Only if Expanding, Pulsatile or with Active Hemorrhage