Definition
- Asymptomatic Adrenal Mass Incidentally Found on Radiographic Examination
Causes
- Nonfunctional Benign Tumor (85-90%)
- Cortical Adenoma (Most Common)
- Ganglioneuroma
- Myelolipoma
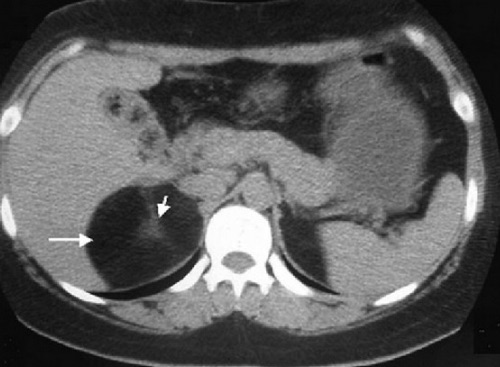
- Adrenal Cyst
- Functional Benign Tumor (10-15%)
- Aldosteronoma
- Cortisol-Secreting Adenoma
- Pheochromocytoma
- Malignancy (2-5%)
- Adrenocortical Carcinoma
- Metastases (Most Common Primary Sites: Lung #1, Breast, Melanoma & Kidney)
Management
- Always Start with Thorough History & Physical Exam
- First Step: Assess Hormonal Function
- Second Step: Assess Risk of Malignancy
- Third Step: Determination of Treatment
Assessment of Hormonal Function
- Plasma Aldosterone & Renin – Evaluate for Hyperaldosteronism (Conn Syndrome)
- 24-Hour Urinary Cortisol or Low-Dose Dexamethasone Suppression Test – Evaluate for Hypercortisolism (Cushing Syndrome)
- Plasma or Urine Metanephrines – Evaluate for Pheochromocytoma
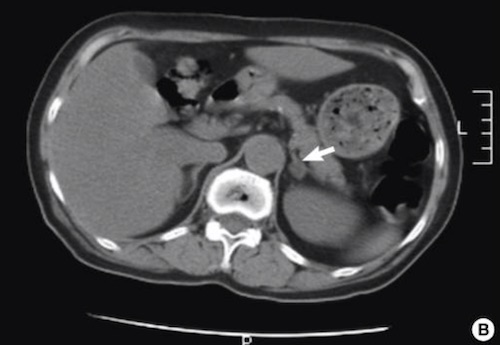
Assessment of Malignancy Risk
- Benign CT Findings:
- Size < 4 cm
- Homogenous
- Precontrast Density < 10 Hounsfield Units (HU)
- Contrast Washout > 50% at 10 Minutes
- Malignant CT Findings:
- Size > 6 cm
- Heterogenous
- Precontrast Density > 20 Hounsfield Units (HU)
- Delayed Contrast Washout
- FNA Biopsy Generally Not Preformed
- Cannot Distinguish Benign Mass from Carcinoma & May Increase Difficulty of Adrenalectomy
- May Be Useful in Distinguishing a Metastatic Tumor – Although Pheochromocytoma Must Always be Ruled Out Prior to Biopsy
Treatment
- Non-Functioning & Benign CT Findings: Observe
- Repeat CT in 3-6 Months, Then Annually for 1-2 Years
- Repeat Biochemical Testing Annually for 5 Years
- Functioning or Malignant CT Findings: Adrenalectomy
- *See Endocrine: Adrenalectomy
- Surgery Indications:
- Hormonally Functional
- Size > 4-6 cm or Rapid Growth
- Known/Suspected Adrenocortical Carcinoma
- Metastatic Tumors
- Approach:
- Laparoscopic Adrenalectomy is Preferred if Able
- Open (Anterior/Transabdominal) Approach if Large > 6 cm or Known/Highly-Suspected Adrenocortical Carcinoma
- *Treatment for Size 4-6 cm is Controversial
Myelolipoma
- Benign Tumor of Adipose & Myeloid Tissue
- Rare Outside of the Adrenal Gland
- Compromise 6-16% of Adrenal Incidentalomas
- Characteristic CT Findings: Well Circumscribed & Hypodense with Attenuation -90 to -120 HU
- Traditionally Treated Conservatively
- Indications for Adrenalectomy: Symptomatic or Large (> 6 cm)