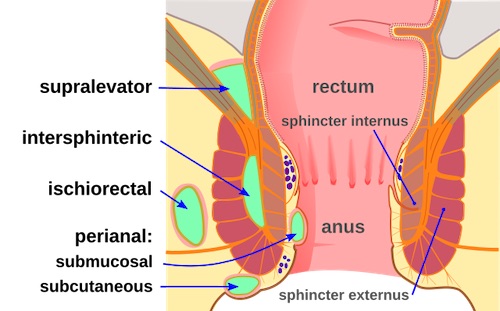
Anorectal Abscess Classification 1
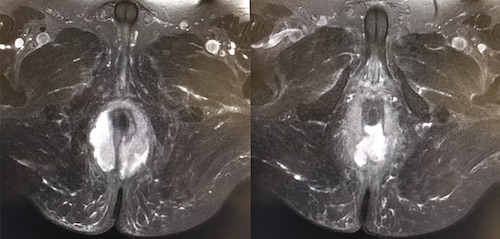
Horseshoe Abscess
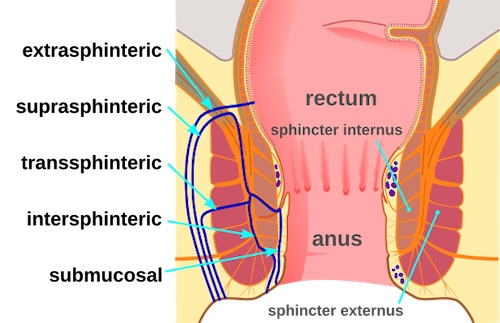
Anorectal Fistula Classification 1
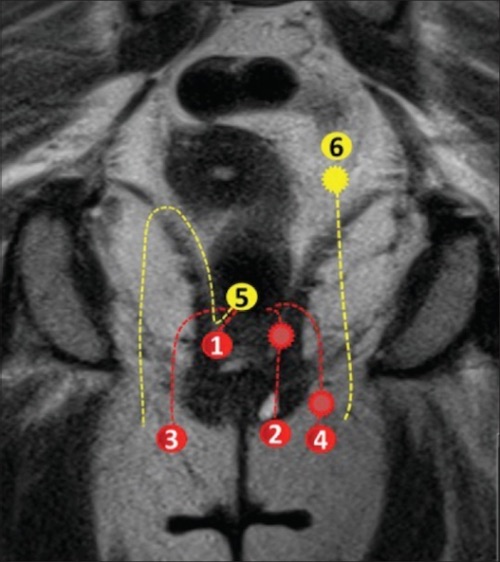
Anorectal Fistula Class by MRI: (1/2) Intersphincteric, (3/4) Transsphincteric, (5) Suprasphincteric, (6) Extrasphincteric 2

Seton 3
Anorectal Abscess Classification 1
Horseshoe Abscess
Anorectal Fistula Classification 1
Anorectal Fistula Class by MRI: (1/2) Intersphincteric, (3/4) Transsphincteric, (5) Suprasphincteric, (6) Extrasphincteric 2
Seton 3