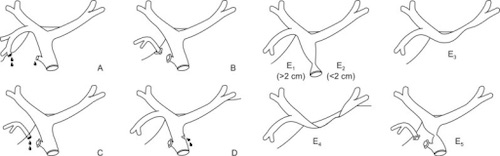
Strasberg Classification (Most Common)
- Type A: Leak from Cystic Duct or Duct of Luschka
- Type B: Occlusion of Aberrant Right Hepatic Duct
- Type C: Leak from Transection of Aberrant Right Hepatic Duct
- Type D: Partial Transection of CBD
- Type E: Complete Transection of CBD
- E1: > 2 cm From Confluence
- E2: < 2 cm From Confluence
- E3: At Confluence but Confluence Intact
- E4: Destruction of Confluence
- E5: Occlusion of CHD & Aberrant Right Hepatic Duct
Bismuth Classification
- Type I: > 2 cm From Confluence
- Type II: < 2 cm From Confluence
- Type III: At Confluence, Confluence Intact
- Type IV: Destruction of Confluence
- Type V: Aberrant Right Hepatic Duct Injury
- With or Without Concomitant CHD Injury
Other Classification Systems
- McMahon Classification
- Stewart-Way Classification
- Hannover Classification
- Mattox Classification