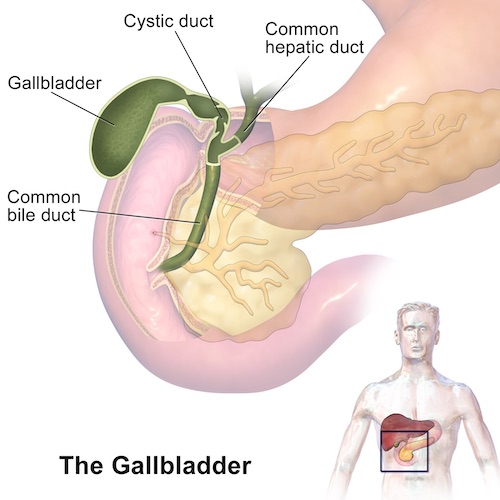
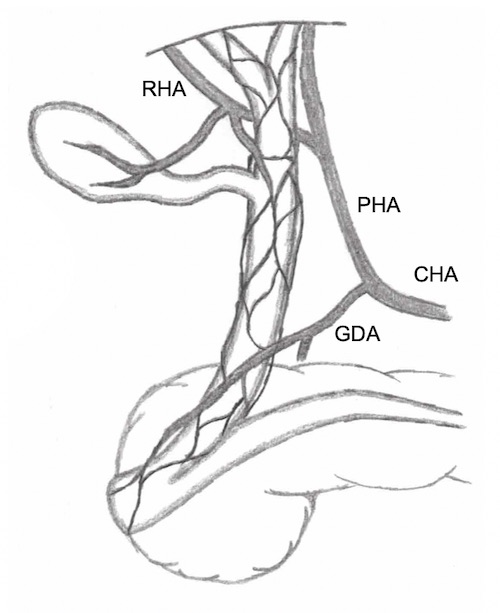
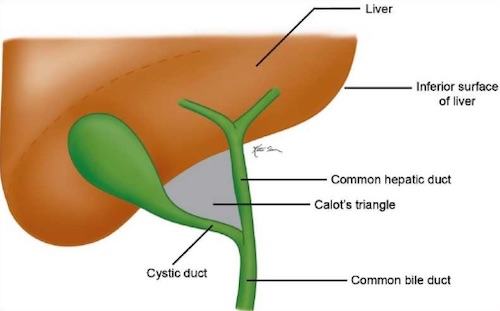
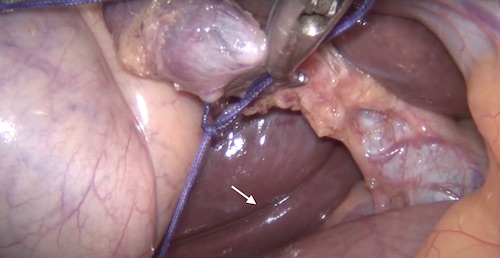
Biliary Tract: Anatomy & Physiology Anatomy Normal SizesCBD < 6-8 mm10 mm After CholecystectomyIncreases 1 mm Every 10 Years After Age 60Gallbladder Wall < 4 mmPancreatic Duct < 4 mmGallbladder AnatomyStructureFundus – Round Distal ProjectionBody – Largest PortionNeck – Tapered Portion Continuous with Cystic DuctLayersMucosa – Columnar EpitheliumNo SubmucosaGallbladder Lies Beneath Liver Segments IV/VBiliary TractLeft & Right Hepatic Ducts Combine to Form Common Hepatic Duct (CHD)Left Haptic Duct is Longer Than RightLeft Haptic Duct is More Likely to Dilate in Distal ObstructionCystic Duct Enters Common Hepatic Duct to Form Common Bile Duct (CBD)Heister Valve – Spiral Valves in Cystic Duct with No Valve FunctionCBD & Pancreatic Duct Unite Outside Duodenal WallTraverse Wall as Single DuctSphincter of OddiMuscular Fibers within Wall of Duodenum Around Ampulla of VaterComponentsSphincter Choledochus (Sphincter of Boyden) – Encircles CBDSphincter Pancreaticus – Encircles Pancreatic DuctInterlocks with Sphincter Choledochus to form Figure-of-EightAccessory StructuresRokitansky-Aschoff SinusesEpithelial Invaginations in Gallbladder WallFrom Increased Pressure (Chronic Cholecystitis)Ducts of LuschkaAccessory Bile Ducts in Gallbladder FossaCan Leak After CholecystectomyVascular SupplyGallbladderCystic Artery – Off Right Hepatic ArteryFound in Triangle of CalotBranches: Superficial & DeepCystic Vein – Into Right Branch of Portal VeinCBDMarginal Arteries at 3-o’clock and 9-o’clock on ERCPSupplyLateral Portion (Proximal): Right Hepatic ArteryMedial Portion (Distal): GDA (Retroduodenal Branches)LymphaticsLie to the Right of CBDNervesParasympathetics – Left Vagus Trunk (Anterior)Sympathetics – Splanchnic & Celiac GanglionsTriangle of CalotBorders:Lateral: Cystic DuctMedial: Common Hepatic DuctSuperior: LiverContents:Cystic ArteryNode of Calot (Cystic Node)First Site of MetsRouviere’s Sulcus – Naturally Occurring Cleft in the Right Lobe of the Liver, Anterior to Segment 1Used as Landmark to Begin Dissection of Calot’s TrianglePresent in 80% of Normal LiversAberrant AnatomyBiliary System:Anatomic Variation Frequency: 30-40%Most Variable Course: Right Posterior Hepatic DuctAnomalies:Trifurcation: Right Posterior Joins with Right Anterior & Left Hepatic Ducts Together (10-11%)Crossover Anomaly: Right Posterior Joins with Left Hepatic Duct (11-15%)Most Common AnomalyOther Anomalies:Right Posterior Joins with Common Hepatic Duct (6%)Right Posterior Joins with Cystic Duct (2%)Right Hepatic Duct Drains into the Cystic DuctAccessory Hepatic Ducts*Multiple Different Classification Systems with Different Types Have Been ProposedVascular System:Cystic Artery Origin Variations: Common Hepatic, Gastroduodenal or SMADouble Cystic Arteries Seen in 10% Gallbladder & Biliary Tract Anatomy 1 Blood Supply of the Biliary Tract Triangle of Calot 2 Rouviere’s Sulcus Physiology BilirubinProductionHgb Breakdown > Heme > Biliverdin > Unconjugated BilirubinUnconjugated BilirubinConjugated in Liver by Glucuronyl Transferase (Adds Glucuronic Acid)Conjugated BilirubinIncreased Water Solubility & Secreted in BileGutConjugated Bilirubin > Urobilinogen > Stercobilinogen > StercobilinBreakdown by Bacteria in Terminal IleumUrobilinogen – ReabsorbedStercobilin – Brown Color of StoolReabsorptionSiteUnconjugated: Passively in Small Intestine & ColonConjugated: Actively in Terminal IleumUrobilinogen > UrobilinUrobilin – Yellow Color of UrineDelta BilirubinConjugated Bilirubin Bound to Albumin18 Day Half-Life – Long Time to Clear When Chronically ElevatedBile ContentsWater (97%)Rapid ConcentrationNaCl – Active Absorption (Na/K ATPase)Water – Passive ResorptionBile Salts (0.7%)Function: Emulsifies Fat, Forming MicellesBile AcidsSource: Cholesterol BreakdownPrimary Bile AcidsCholic & Chenodeoxycholic Mn Produced in LiverSecondary Bile AcidsDeoxycholic & LithocholicTransformed by Bacteria in GutRecycled Through Enterohepatic CirculationBile Salt: Bile Acid (Primary or Secondary) Conjugated with Taurine & GlycineImprove Water SolubilityAllow Secretion in BileCholecystectomy Effects:Minimal Effect on Bile Acid SecretionIncreased Enterohepatic Bile Salt CirculationFats (0.5%)LecithinPhospholipidFunction: Emulsifies Fat & Solubilizes CholesterolCholesterolFatty AcidsBilirubin (0.2%)*See AboveInorganic SaltsHormonesBile ExcretionIncreased: Secretin #1, CCK, Parasympathetic (Vagus) InputDecreased: Somatostatin, Sympathetic (Splanchnic) InputGallbladder ContractionCCK: Constant/Steady ContractionMotilin: Stimulates Contraction in Fasting StateParasympathetic (Vagus) Input Stimulates ContractionSphincter of Oddi ControlMorphine: ContractsGlucagon: Relaxes*See General Abdomen: GI Hormones Mnemonic Primary vs Secondary Bile Salts“C-Comes First”Cholic & Chenodeoxycholic are Primary Bile SaltsDeoxycholic & Lithocholic are Secondary Bile Salts References Wikimedia Commons (License: CC BY-SA-4.0)Perera E, Bhatt S, Dogra VS. Cystic duct remnant syndrome. J Clin Imaging Sci. 2011;1:2. (License: CC BY-NC-SA-3.0)