Specific Lymph Node Concerns
- Suspicious Lymph Node Found on Physical Exam: US & FNA Prior to Surgery
- Supraclavicular Lymph Node: Chemotherapy, Radiation Therapy & Resect the Primary Breast Lesion
- Resect Lymph Node Only if Not Fully Treated
Lymph Node Metastases
- Isolated Tumor Cells (ITC): < 0.2 mm
- Micrometastases: 0.2-2.0 mm
- Slightly Worse Prognosis
- May Predict Recurrence (Debated)
- Micrometastases: ≥ 2.0 mm
- Significantly Effects Survival
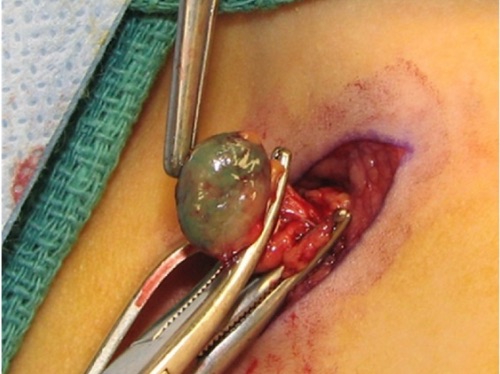
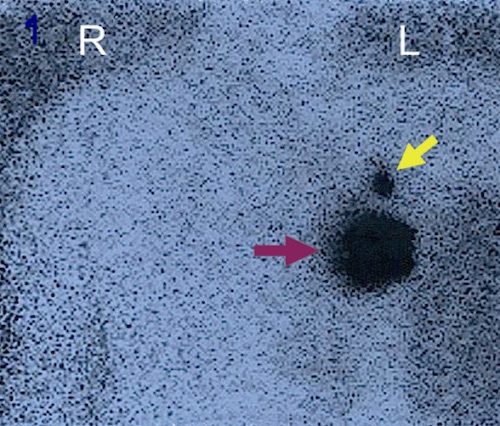
Sentinel Lymph Node Biopsy (SLNB)
- Definition: Surgical Removal of Axillary Sentinel Lymph Nodes
- Indications:
- Invasive Carcinoma if Early (T1 or T2) with Clinically Negative Nodes
- DCIS if Mastectomy is Performed
- Contraindications:
- Clinically Positive Nodes
- Inflammatory Breast Cancer
- Locally Advanced Disease (T3 or T4)
- May Still Consider SLNB for T3 Disease (Debated)
- Debated Contraindications
- Large Tumors (T3)
- After Neoadjuvant Chemotherapy
- Prior Axillary Surgery
- False Negative Rate: 5-10%
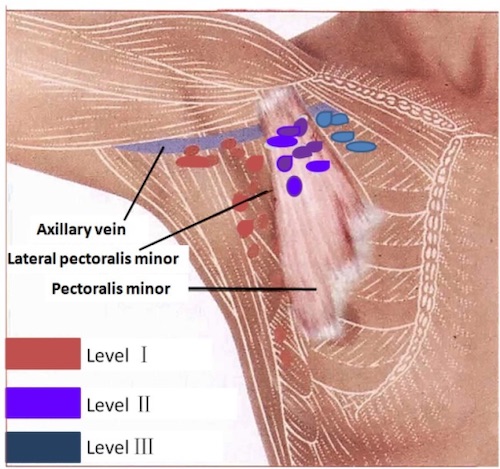
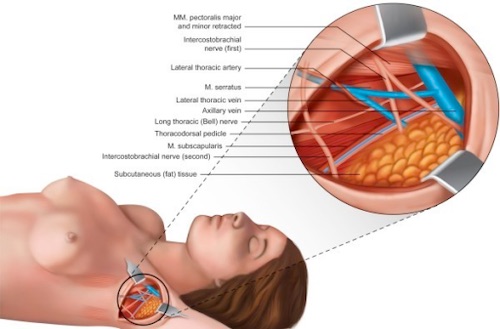
Axillary Lymph Node Dissection (ALND)
- Definition: Surgical Removal of Axillary Lymph Node Levels I & II
- Does Not Include Level III
- Indications:
- If SLNB is Contraindicated
- After SLNB If:
- No Radiotracer/Dye is Found (Rate < 5%)
- ≥ 3 Positive Lymph Nodes are Pathologically Confirmed (ACOSOG Z0011 Trial)
- *Specifically Referring to Lumpectomy
- Any Positive Lymph Nodes After a Mastectomy – Debated
Complications
- Decreased Arm Range-of-Motion (40%) – Most Common Complication After Axillary Surgery
- Infection (7%)
- Hematoma (2-10%)
- Seroma
- Nerve Injury (< 1%)
- Arm Swelling
- Sudden/Early: Concern for Axillary Vein Thrombosis
- Slow/Late: Concern for Lymphatic Fibrosis
- Lymphedema
- SLNB Risk: < 5%
- ALND Risk: 20%
- Stewart-Treves Syndrome