Basics
- Laparoscopic Removal of the Gallbladder
Procedure
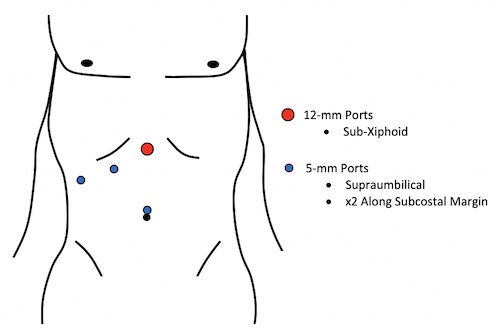
- Access Abdomen – x4 Trocars (Periumbilical & x3 Subcostal)
- Expose Gallbladder
- Position Reverse Trendelenburg & Left Side Down
- Retract Fundus Cephalad
- Retract Body Laterally
- *If Difficult to Grab – Consider Decompression by Needle-Aspiration
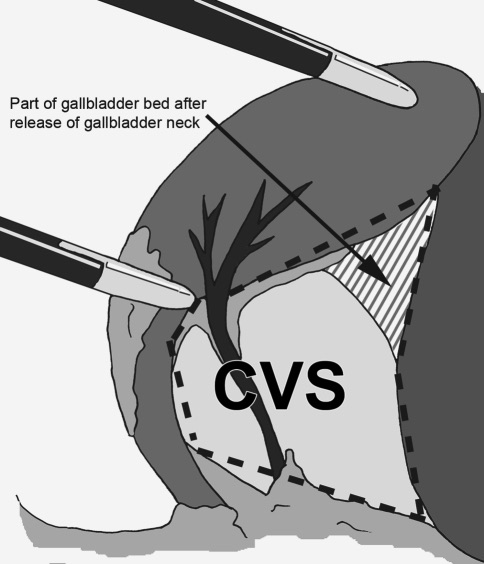
- Expose the Critical View of Safety
- Divide Cystic Duct & Cystic Artery
- Two Clips Away from the Gallbladder & One Clip Near the Gallbladder
- *Terms Proximal & Distal to the Gallbladder are Generally Discouraged Due to Variability in Meaning
- Dissect Gallbladder from Liver Bed & Remove
- Ensure Hemostasis
- Close Incision Sites
Considerations
- Critical View of Safety – SAGES Safe Cholecystectomy Program
- Only Two Structures Entering Gallbladder (Cystic Artery/Duct)
- Triangle of Calot Cleared of All Fat & Fibrous Tissue
- Lower Third of Gallbladder Separated from Liver
- Encouraged Liberal Use of Intraoperative Cholangiography (IOC)
- Especially in Difficult Cases with Unclear Anatomy
- Routine Use Unnecessary
- If Approaching a Zone of Significant Risk – Finish by a Safe Method:
- Conversion to Open
- Subtotal Cholecystectomy After Removal of All Stones
- Cholecystostomy Tube
- Low Threshold for Calling in Help of Other Experienced Surgeons
Intraoperative Cholangiogram (IOC) & Bile Duct Exploration
Laparoscopic Complications
- Retained Stone
- Stone Retained in Common Bile Duct
- If Intraoperative Concern: Leave T-Tube
- Wait 4-6 Weeks for Tract to Mature Before Instrumentation/Cholangiogram
- If CBD Stone Still Present: Extract Through T-Tube
- Best Predictor: Persistent High Total Bilirubin
- Spilled Stone
- Stone Spilled into the Peritoneal Cavity
- Can Cause Abscess
- Tx: Laparoscopic Drainage & Stone Removal
- Percutaneous Drain Will Recur
- Biliary Injury (0.26-0.60%)
- Bleeding (0.11-1.97%)
- Abscess (0.14-0.30%)
- Bowel Injury (0.14-0.35%)
Conversion to Open Procedure
- Rate of Conversion: Generally Reported as 5-10%
- *Modern Rates Lower and Decreasing
- Risks for Conversion: Elderly, Emergency Status, Male, Low Albumin & Previous Abdominal Surgery
- Modern Surgeons are Generally More Comfortable with Laparoscopic Approaches with Conversion Often Providing Less Benefit
- All Surgeons, However, Should Be Comfortable Opening if Necessary