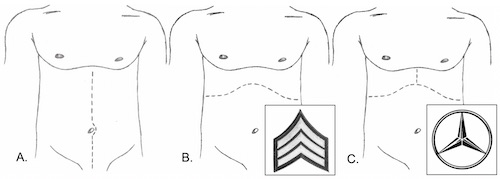
General Exploration
- Once Bleeding Temporarily Controlled
- Order of Exploration:
- 1. Inframesocolic
- 2. Supramesocolic
- 3. Lesser Sac
- 4. Retroperitoneum
- *Some Report Different Orders of Exploration – Exact Order is Not as Important as Making Sure to Preform it the Same Way Every Time & to Not Miss Any Injuries
Inframesocolic Exploration
- Lift Transverse Colon Cranially
- Run Bowel from Ligament of Treitz to Rectum
- Transverse Colon & Hepatic/Splenic Flexures are Notorious for Missed Injury
- Inspect Bladder & Pelvis
Supramesocolic Exploration
- Pull Transverse Colon Caudally
- Inspect from Right-to-Left
- Palpate Liver, Gallbladder & Right Kidney
- Then Stomach & Duodenum
- Finally, Palpate Spleen & Left Kidney
Lesser Sac Exploration
- Bluntly Dissect Through the Greater Omentum (Left Side Less Vascular)
- Inspect Posterior Stomach & Pancreas
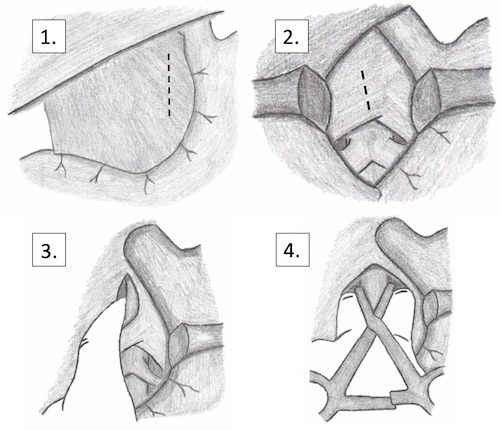
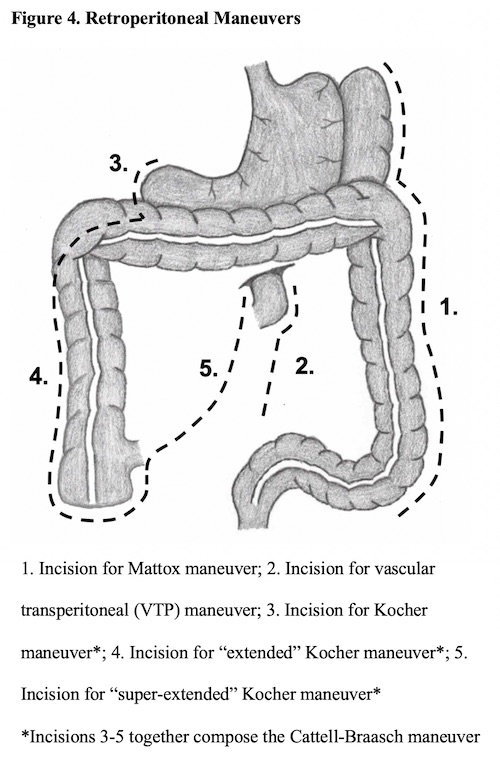
Retroperitoneum Exploration
- Keep Retroperitoneal Exploration Targeted & Limited
- Clinical Suspicion Based on Missile Trajectory or Presence of Hematoma
- Maneuvers: