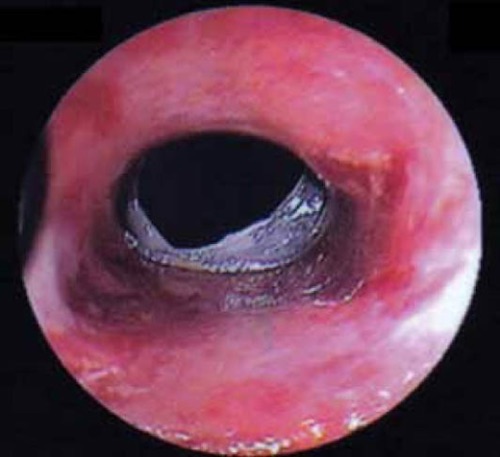
Dysphagia Lusoria (Bayford-Autenrieth Dysphagia)
- Latin for Dysphagia by a “Freak of Nature”/“Jest of Nature”
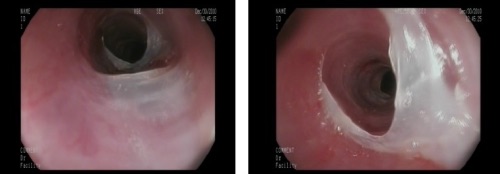
- Definition: Dysphagia Caused External Compression from a Birth Defect of the Aortic Root Anatomy
- Risk Factors: Down’s Syndrome & Congenital Heart Disease
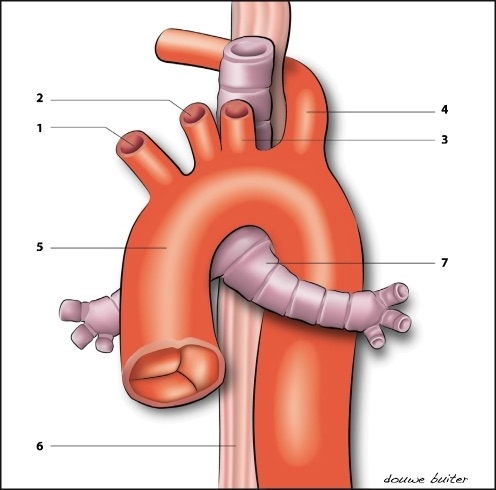
- Abnormalities:
- Aberrant Right Subclavian Artery off the Descending Aorta (After Left Subclavian)
- Most Common Cause
- The Primary Abnormality Described in the Literature
- 60% Associated with an Aneurysm of the Proximal Portion (“Kommerell Diverticulum”)
- Persistent Right Aortic Arch with Aberrant Left Subclavian Artery
- Tortuous or Aneurysmal Thoracic Aorta
- Enlarged Left Atrium
- Dx: CT Angiogram
- Barium Esophagram Suggests but is Not Diagnostic
- Tx:
- Mild-Moderate Sx: Dietary & Lifestyle Modifications
- Eat Slower with Small Bites & Chewing Well
- Severe Sx: Vascular Reconstruction
- If from Aberrant Right Subclavian Artery – Divide & Translocate the Distal Subclavian to the Aortic Arch or Right Common Carotid