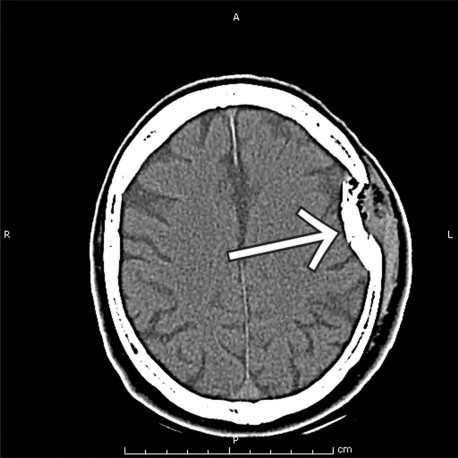
Skull Fracture 1
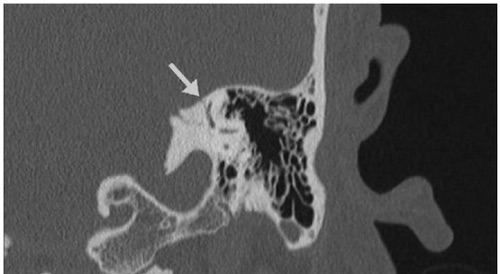
Temporal Bone Fracture 2

Racoon Eyes 3

Battle Signs 4

Frontal Sinus Fracture 5

Nasal Fracture 6

Orbital Blowout Fracture 7
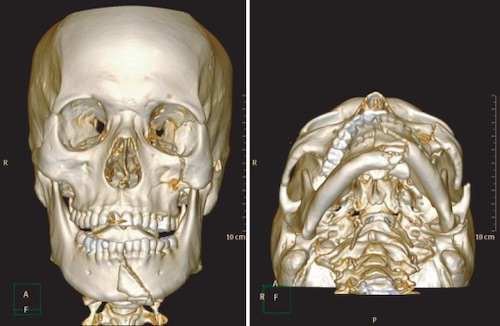
ZMC & Mandible Fracture 8
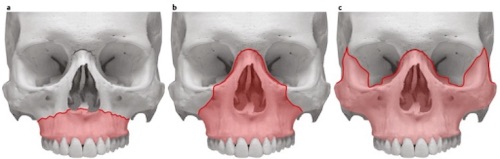
Le Fort Fractures; (a) Type I, (b) Type II, (c) Type III 9

Facial Laceration of the Vermillion Border 10

Auricular Hematoma 11