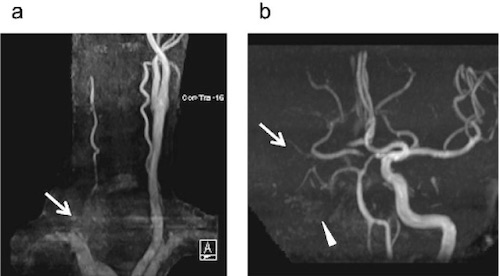
Internal Carotid Artery – Penetrating Injury
- Tx: Surgery
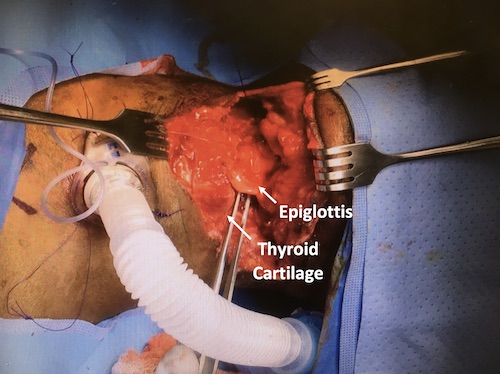
- Surgical Repair Options:
- Primary Arteriorrhaphy
- Patch Angioplasty
- End-to-End Anastomosis
- Vein or PTFE Graft
- ECA Transposition to Injured ICA
- Ligation Indications (High CVA Risk: 75-80%):
- Unstable
- Very Severe Neck Injury
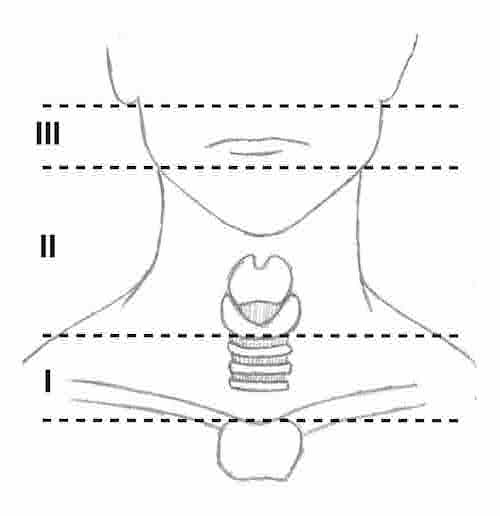
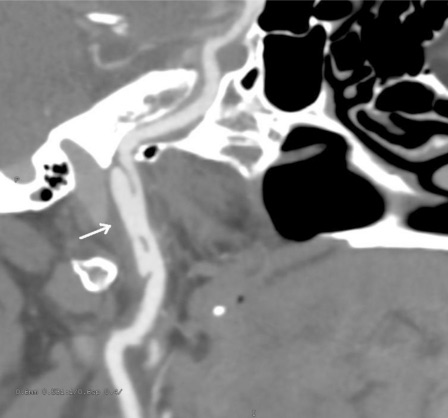
- Zone III ICA Injury at Skull Base
External Carotid Artery
Internal Jugular Vein
- Transverse Venorrhaphy if Able
- Major Hemorrhage/Unstable: Ligate
Subclavian/Axillary Artery
- Tx: Endovascular vs Open Repair
- Pseudoaneurysm: Endovascular Stent
- Laceration > 50%/Transection: Open Repair