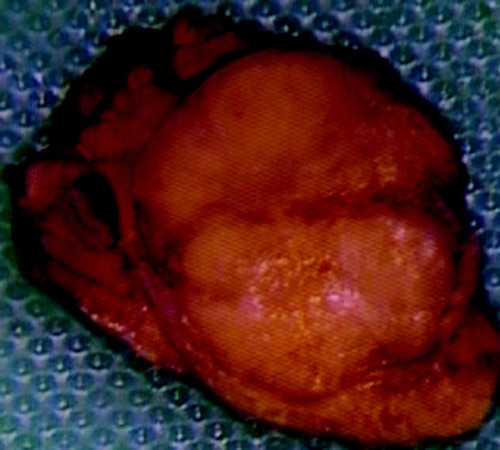
Insulinoma 1
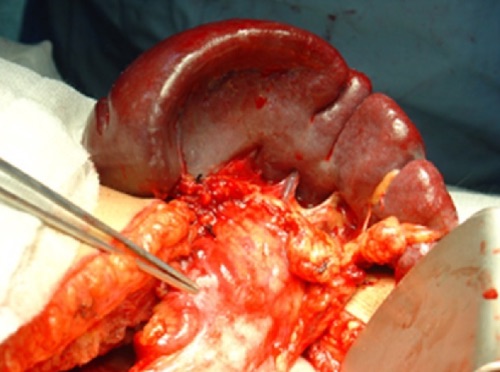
Glucagonoma in Pancreatic Tail 2

Necrolytic Migratory Erythema (NME) 3
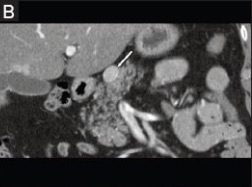
PNET on CT 4
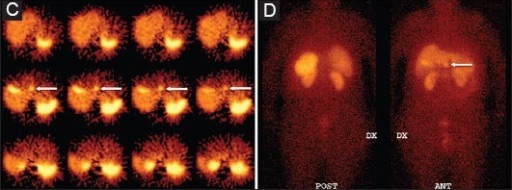
PNET on SRS 4
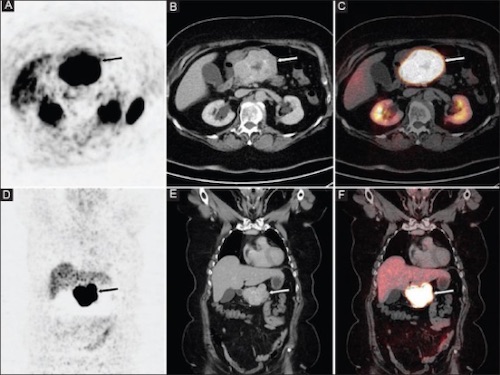
PNET on Functional PET 4

PNET on EUS 4
#6 – The Number of the Pancreas
#6 – The Number of the Pancreas
Insulinoma 1
Glucagonoma in Pancreatic Tail 2
Necrolytic Migratory Erythema (NME) 3
PNET on CT 4
PNET on SRS 4
PNET on Functional PET 4
PNET on EUS 4
#6 – The Number of the Pancreas
#6 – The Number of the Pancreas