
Axillobifemoral Bypass 1

Femorofemoral Bypass 2
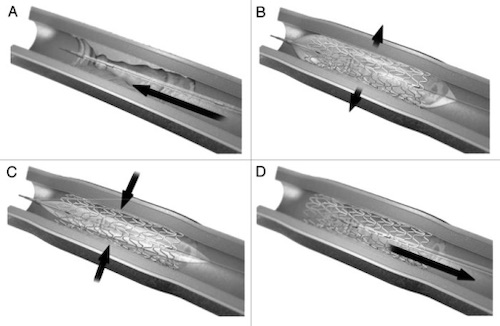
Endovascular Stent Placement; (A) Stent Mounted on Catheter, (B) Balloon Inflated and Stent Expanded, (C) Balloon Deflated, (D) Catheter Removed 3

Femoral Endarterectomy 4
Axillobifemoral Bypass 1
Femorofemoral Bypass 2
Endovascular Stent Placement; (A) Stent Mounted on Catheter, (B) Balloon Inflated and Stent Expanded, (C) Balloon Deflated, (D) Catheter Removed 3
Femoral Endarterectomy 4