Goals for Appropriate Dosing: BP < 130/80, Mildly Orthostatic & Dry Nasal Mucosa/”Stuffy Nose”
Alternative Regimens:
Selective α-Blockers (Prazosin, Doxazosin or Terazosin)
CCB (Nifedipine, Verapamil, Nicardipine or Amlodipine)
Second Step: β-Blockade if Needed for Reflex Tachycardia
Wait to Start ≥ 2 Days After Initiation of α-Blockade
Additional Considerations:
High-Salt Diet to Restore Fluid Volume
Metyrosine (Tyrosine Hydroxylase Inhibitor) May Be Used to Control Hypertension from Unresectable Tumors – Use Limited Due to Significant Side Effects
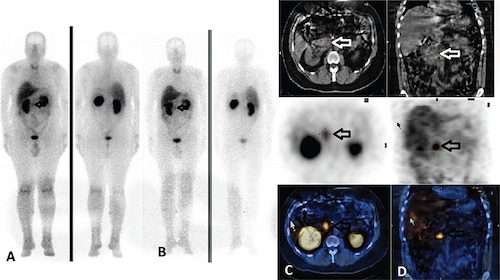
Pheocromocitoma on MIBG Scan 1
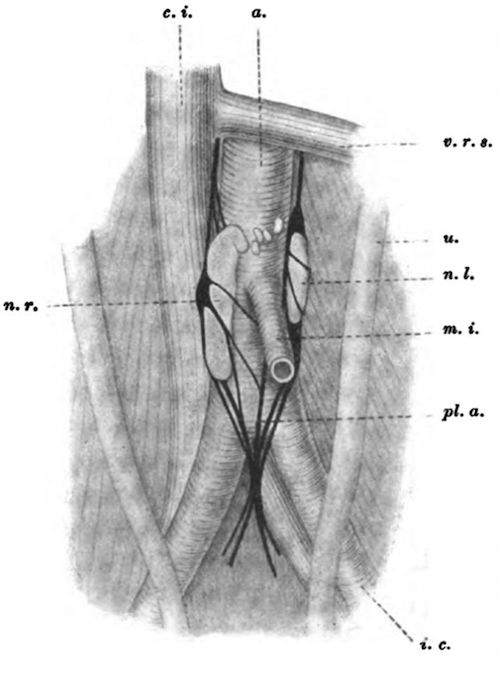
Organ of Zuckerkandl 2
Paraganglioma of the Organ of Zuckerkandl 3
Mnemonics
Order of Blockade
A Before B
References
Arıcan P, Okudan Tekin B, Naldöken S, Şefizade R, Berker D. A Family with Von Hippel-Lindau Syndrome: The Findings of Indium-111 Somatostatin Receptor Scintigraphy, Iodine-123 Metaiodobenzylguanidine Scintigraphy and Single Photon Emission Computerized Tomography. Mol Imaging Radionucl Ther. 2017 Feb 5;26(1):38-42.(License: CC BY-4.0)
Zuckerkandl E 1901 Ueber Nebenorgane des Sympathicus im Retroperitonaealraum des Menschen.Verhandlungen der Anatomischen Gesellschaft. 14:95–107
Gannan E, van Veenendaal P, Scarlett A, Ng M. Retroperitoneal non-functioning paraganglioma: A difficult tumour to diagnose and treat. Int J Surg Case Rep. 2015;17:133-5.(License: CC BY-NC-ND-4.0)