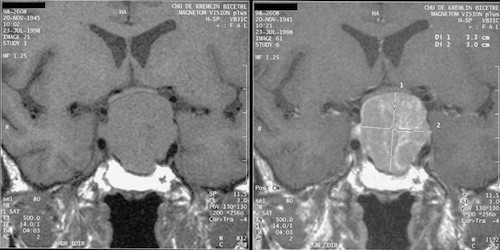
Pituitary Apoplexy (“Sudden Attack”)
- Sudden Hemorrhage or Infarction of the Pituitary Gland
- Risk Factors:
- Pituitary Adenoma (Most Common)
- May Occur After Radiation Therapy
- Hypertension
- Major Surgery
- Medications
- Head Trauma
- Presentation:
- Sudden Excruciating Headache
- Diplopia & Decreased Visual Acuity
- Altered Mental Status
- Nausea & Vomiting
- Hormone Deficiencies (Minority are Clinically Significant)
- Hemodynamic Shock – From ACTH Loss
- Diagnosis: MRI/CT
- Treatment: Steroids & IVF
- May Require Surgical Decompression for Severe Vision Changes or Neurologic Symptoms
Sheehan Syndrome
- Pituitary Gland Infarction Due to Postpartum Hemorrhage (Typically Large Losses)
- Pituitary Hypertrophies While Pregnant
- Presentation:
- Lactation Failure (Most Common Symptom)
- Failure to Resume Menses/Amenorrhea
- Lethargy & Fatigue
- Weight Loss
- Hypothyroid
- Treatment: Hormone Replacement
Nelson Syndrome
- Pituitary Gland Hypertrophy After Bilateral Adrenalectomy for Cushing Disease
- Loss of HPA Axis Feedback Causes Increased CRH/ACTH Production
- Generally Occurs 1-5 Years Postoperatively
- Presentation:
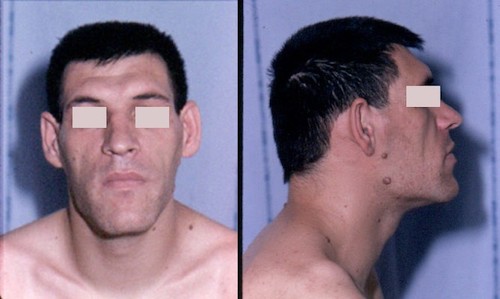
- Hyperpigmentation (Most Overt Symptom)
- From ACTH Conversion to CRH
- May Cause a Prominent Linea Nigra from the Pubis to Umbilicus
- Headache
- Diplopia & Decreased Visual Acuity
- Amenorrhea
- Diagnosis: Increased ACTH After Surgery & MRI
- Primary Treatment: Transsphenoidal Resection
- If Surgery Not an Option: Radiation or Medical Therapy
Craniopharyngioma
- Solid/Cystic Tumor from the Remnant of Rathke’s Pouch
- Rathke’s Pouch: Ectoderm That Becomes Anterior Pituitary
- Presentation (From Mass Effect):
- Headache
- Bitemporal Hemianopia – From CN II Compression
- Mildly Decreased Hormone Release
- Diagnosis: MRI/CT
- Primary Treatment: Transsphenoidal Resection
- May Require Adjuvant Radiation for Residual Disease