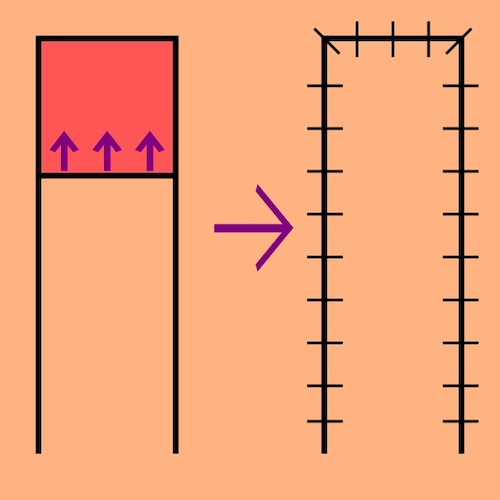
Advancement Flap 1
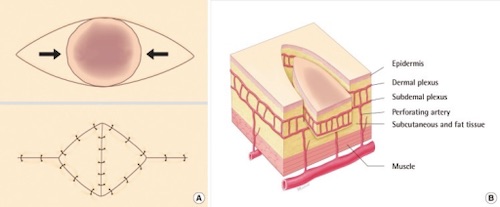
V-Y Advancement Flap 2
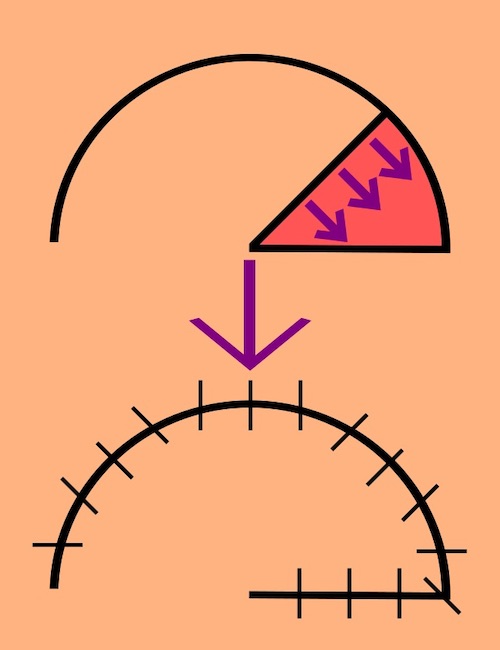
Rotational Flap 1
![]()
Transposition Flap 1
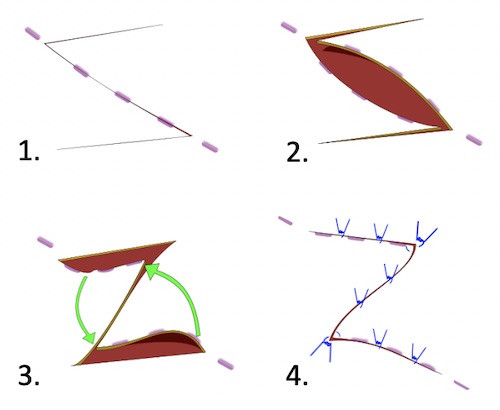
Z-Plasty 3

Skin Graft Dermatome 4

Dermacarrier & Mesher 5

Meshed STSG 6
Advancement Flap 1
V-Y Advancement Flap 2
Rotational Flap 1
![]()
Transposition Flap 1
Z-Plasty 3
Skin Graft Dermatome 4
Dermacarrier & Mesher 5
Meshed STSG 6