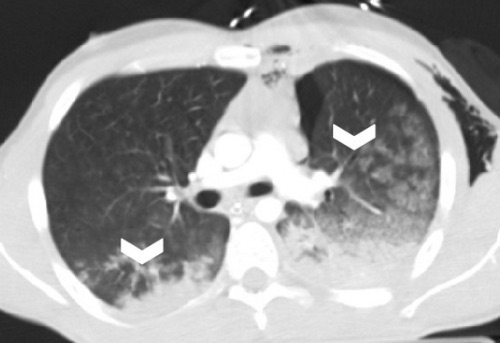
Pulmonary Contusion 1

Pulmonary Laceration; Curved Arrow – Pneumatocele, Straight Arrow – Hematocele 1
PTX

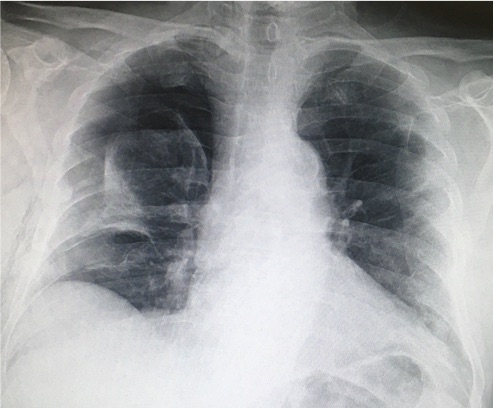
Deep Sulcus Sign (Right) on Supine CXR 2
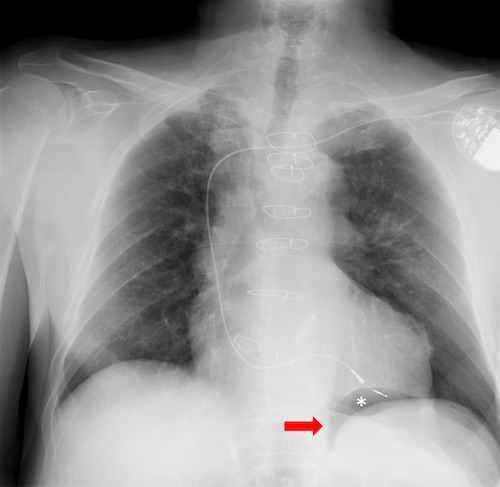
Double Diaphragm Sign (Astrisk) on Supine CXR 3
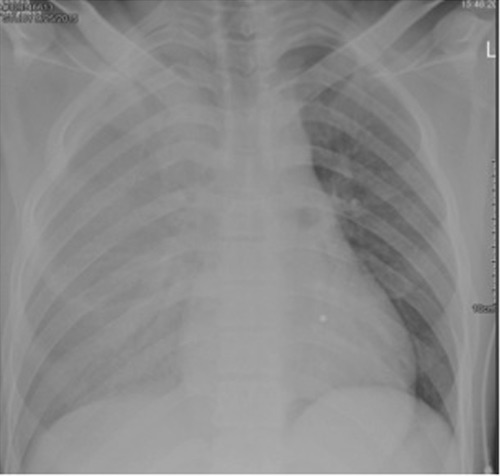
HTX 4
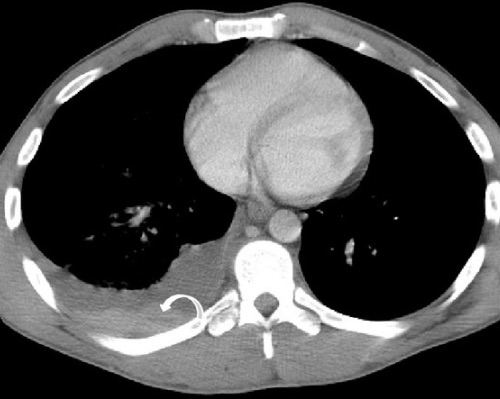
Retained HTX with Hematocrit Sign 1
![]()
Left Main Bronchus Transection 5
![]()
Bronchial Transection 6