AAST Thoracic Vascular Injury Scale
Basics
- Thoracic Vascular Injury Causes 50% of All Trauma Deaths
- Most Common Large Vessel Injury:
- Stab Wound: Ascending Aorta
- GSW: Descending Aorta
- Blunt: Aortic Isthmus (Just Beyond Left Subclavian Takeoff)
- Postoperative Paraplegia Incidence:
- Open Surgery: 8%
- Endovascular: 1%
Blunt Aortic Injury (BAI)
- Vancouver Classification:
- Grade I: Intimal Flap, Thrombus or Intramural Hematoma < 1 cm
- Grade II: Intimal Flap, Thrombus or Intramural Hematoma ≥ 1 cm
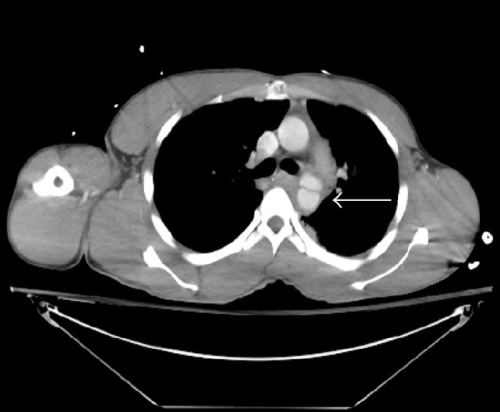
- Grade III: Pseudoaneurysm without Contrast Extravasation
- Grade IV: Free Rupture with Contrast Extravasation
- Thoracic Aorta Transection
- Cause: Rapid Deceleration
- Highest Risk Sign: 1st/2nd Rib Fracture
- Most Common Site: Ligamentum Arteriosum
- Dx: CXR, Then CTA (If Stable)
- Tx:
- Grade I: Anti-Impulse Control
- Goal SBP ≤ 100 mmHg
- Goal HR ≤ 100
- Grade II-IV: Repair
- Stable:
- Ascending or Arch: Open Repair
- Descending: TEVAR (Thoracic Endovascular Aortic Repair)
- Vs Open Repair – Lower Mortality, Blood Loss & Paraplegia Risk
- May Require Coverage of Left Subclavian Depending on Location
- Unstable: Open Repair
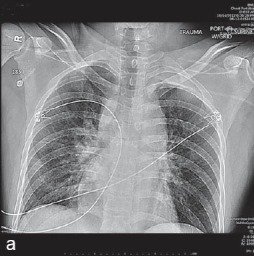
CXR Findings Suggestive of Vascular Injury
- Indistinct Aortic Knob
- Wide Mediastinum > 8 cm
- Left Main Bronchus Depression > 140 Degrees
- Deviation of NG/ET Tubes to the Right
- Massive Hemothorax