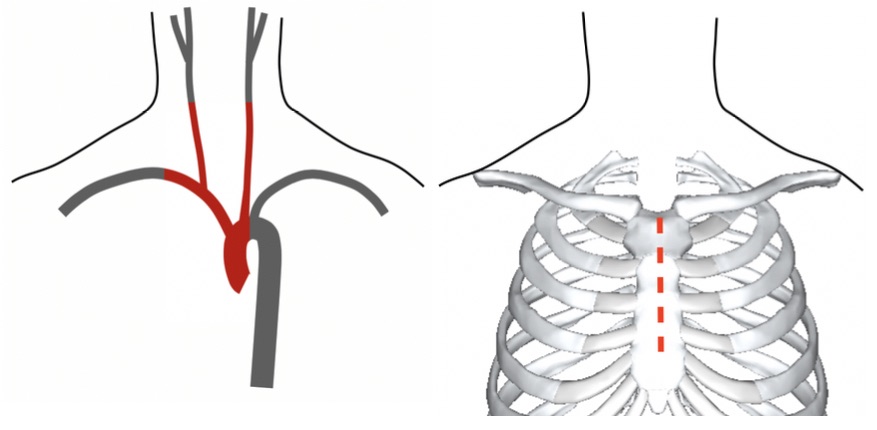
Exposure by Median Sternotomy
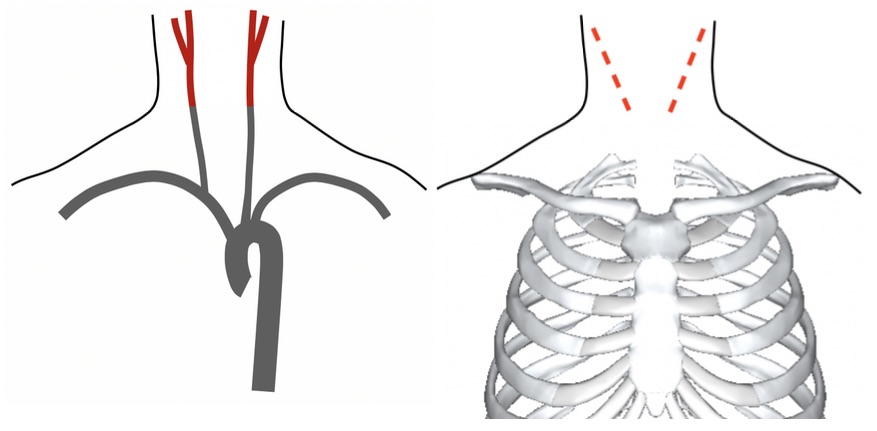
Exposure by Cervical Incision
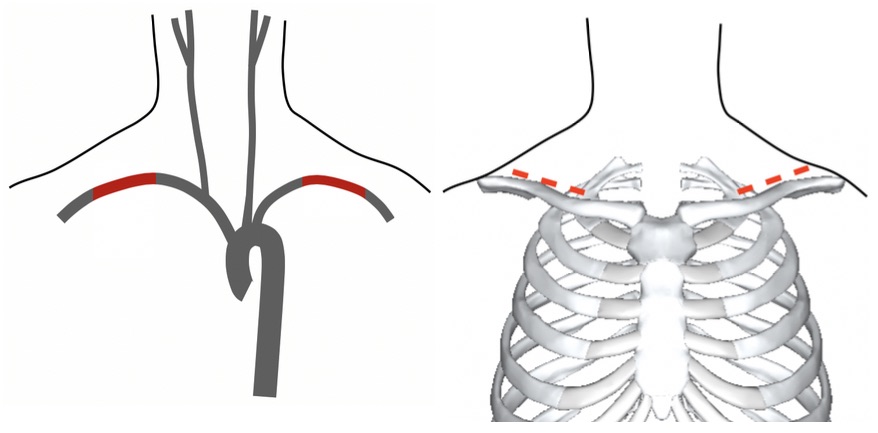
Exposure by Supraclavicular Incision
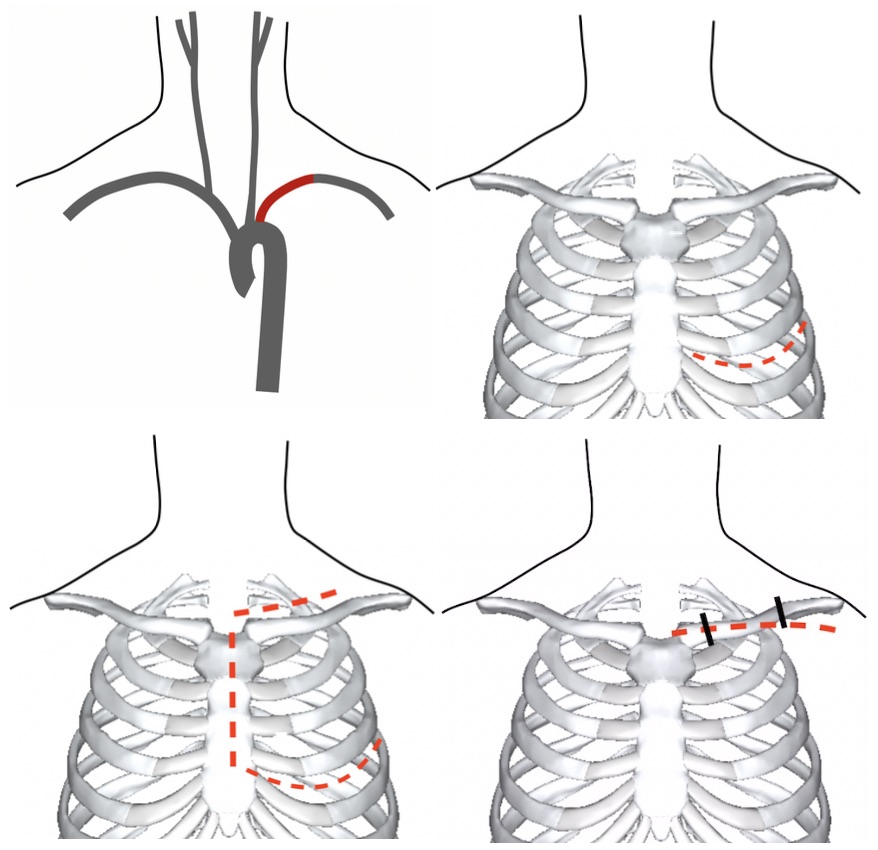
Access to Left Subclavian (Thoracotomy, Trap Door & Clavicular Incisions)
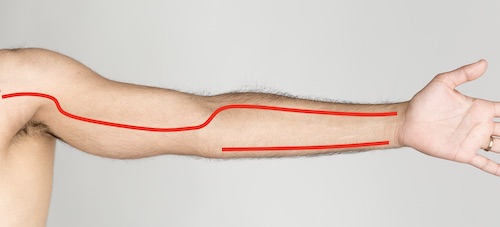
Upper Extremity Incisions
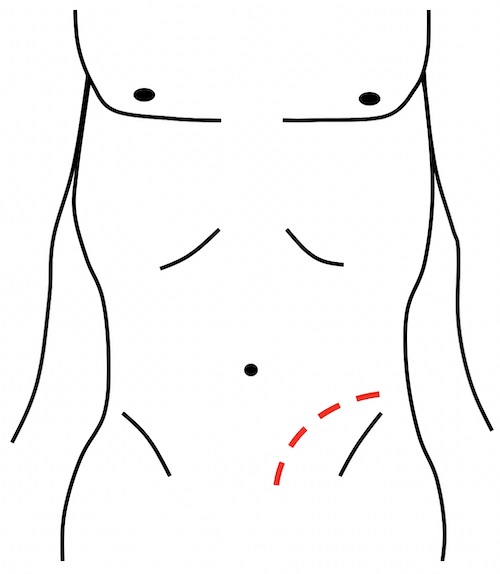
Iliac Exposure
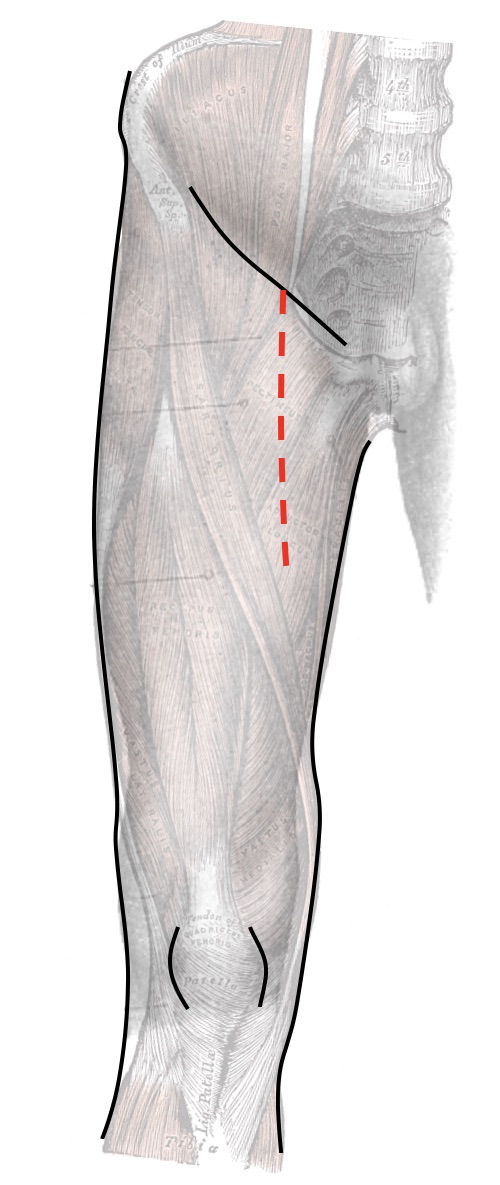
Proximal Femoral Exposure
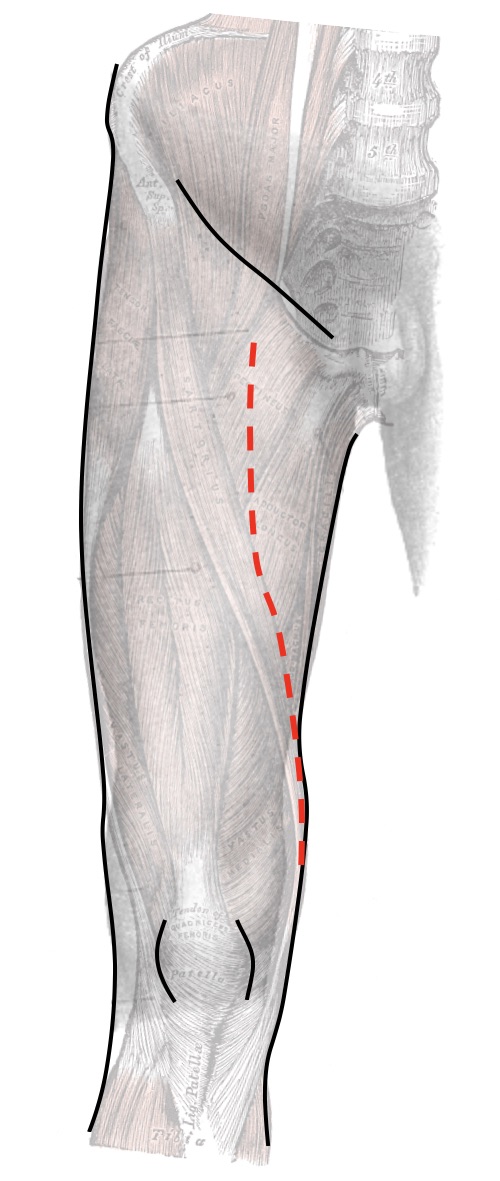
Distal SFA Exposure
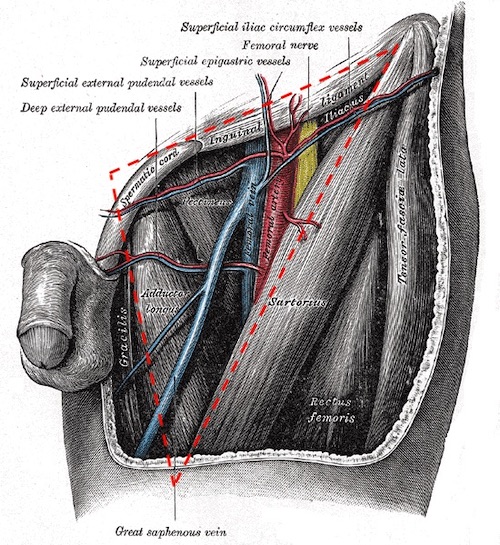
Femoral Triangle
Popliteal Artery Exposure