Stomach: Vagotomy & Pyloroplasty
Vagotomy
Effects
- Primary Goal: Diminished Cholinergic Stimulation of Parietal Cells
- Decreased Gastric Acid Secretion
- Compensatory Increased Serum Gastrin
- Branch Effects:
- Distal Portions: Impaired Distal Gastric Motility & Pylorus Relaxation
- Increased Emptying of Solids
- Decreased Emptying of Liquids
- Celiac Branch: Impaired Small Intestine Motility
- Hepatic Branch: Impaired Gallbladder Motility
- Distal Portions: Impaired Distal Gastric Motility & Pylorus Relaxation
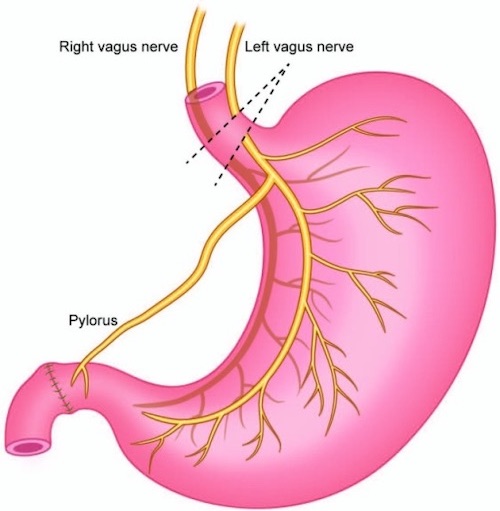
Truncal Vagotomy
- Divides Anterior & Posterior Vagal Trunks as They Emerge Below the Diaphragm
- Lowest Recurrence Rate but More Complications
- Addition of Antrectomy Has the Lowest Recurrence Rate
- Procedure:
- Incise Peritoneum of GE Junction Horizontally from Right to Left Crura
- Bluntly Encircle the Esophagus
- Include Vagal Nerves
- Stay Wide to Avoid Esophageal Injury
- Resect a 1-2 cm Segment of Each Trunk with Clips Placed at the Proximal/Distal Ends
- Posterior Trunk Often Branches Before Entry into Abdomen
- Mare Sure to Include the Criminal Nerve of Grassi Off the Posterior Trunk
- Requires a Concurrent Gastric Emptying Procedure (Pyloroplasty or Gastrojejunostomy)
Selective Vagotomy
- Divides Anterior & Posterior Vagal Trunks After Takeoff of the Hepatic (Anterior) & Celiac (Posterior) Branches
- Now Rarely Used – More Historical
- Attempt Was to Prevent Postvagotomy Diarrhea & Biliary Stasis Although Studies Have Shown No Difference in Diarrhea
- Procedure:
- Incise Peritoneum of GE Junction Horizontally from Right to Left Crura
- Bluntly Encircle the Esophagus
- Include Vagal Nerves
- Stay Wide to Avoid Esophageal Injury
- Resect a 1-2 cm Segment of Each Trunk Distal to the Celiac & Hepatic Branches
- Place Clips at the Proximal/Distal Ends Prior to Resection
- Consider Resection of the Criminal Nerve of Grassi After it Branches Off the Posterior Trunk
- Still Requires a Concurrent Gastric Emptying Procedure (Pyloroplasty or Gastrojejunostomy)
Highly-Selective (Proximal Gastric/Parietal Cell) Vagotomy
- Divides Individual Fibers Along the Lesser Curvature
- Preserves: Vagal Trunks, Hepatic Branch, Celiac Branch & Distal “Crow’s Foot”
- Comparison to Truncal Vagotomy:
- Similar Reduction in Acid Secretion
- Highest Recurrence Rate
- Significantly Decreased Complication Rates
- Normal Emptying of Solids with Some Minimal Rapid Emptying of Liquids
- Lower Incidence of Dumping Syndrome
- Procedure:
- Start 6 cm Proximal to Pylorus on the Anterior Wall of the Stomach
- Work Up the Anterior Lesser Curvature Dividing End Blood Vessels & Vagal Branches
- Identify & Protect the Anterior Nerve of Larajet as it Approaches the GE Junction
- Divide Peritoneum Over the Lower Esophagus to Identify the Anterior & Posterior Vagal Trunks
- Identify & Divide the Posterior Branches in a Similar Fashion
- Consider “Peritonealizing” the Lesser Curvature
- Approximate the Anterior & Posterior Gastric Walls with Interrupted Sutures
- Will Prevent Perforation from Necrosis of the Denuded Lesser curvature
- Variations:
- Hill-Baker Procedure – Posterior Truncal Vagotomy & Anterior Highly-Selective Vagotomy
- Taylor Procedure – Posterior Truncal Vagotomy & Anterior Seromyotomy of Lesser Curvature
Complications
- Recurrent Ulcers
- Highly-Selective Vagotomy: 15%
- Truncal Vagotomy: 10%
- Truncal Vagotomy with Antrectomy: 2% (Lowest)
- Postvagotomy/Osmotic Diarrhea (30%)
- Most Common Complication
- Cause: Sustained Migrating Motor Complex (MMC) – More Bile into Colon
- No CV Sx as Seen in Dumping Syndrome
- Tx: Cholestyramine & Loperamide
- Dumping Syndrome
- Gastroparesis
- *See Stomach: Gastric Emptying Diseases
- If All Other Tx Options Fails May Consider Near-Total Gastrectomy & Roux-en-YGastrojejunostomy
- Dysphagia (1-3%)
- Cause: Fibrosis & Lower Esophageal Denervation
- Onset Weeks-Months After
- Tx: Endoscopic Dilation
- If Fails: Myotomy
Truncal Vagotomy 1
Pyloroplasty
Basics
- General Indications:
- Peptic Ulcers, Preformed Concurrently with Vagotomy
- Gastroparesis Failed Conservative Measures
- Procedures Similar to Sphincteroplasty
Heineke-Mikulicz Pyloroplasty
- Most Common Approach
- Procedure:
- Kocher Maneuver to Mobilize Duodenum
- Make a Longitudinal Incision Through the Pylorus
- Start on Stomach 2-3 cm Proximal to Pylorus
- End on Duodenum 2-3 cm Distal to Pylorus
- Close the Incision Transversely
- Use Traction Sutures at the Midpoints to Pull and Assist in Closure
- Close in 1-2 Layers
- Goal is Complete Inversion with Good Serosa-to-Serosa Approximation
Finney Pyloroplasty
- Used if Significant Scarring & Narrowing of the Duodenal Bulb Prohibiting Heineke-Mikulicz
- Procedure:
- Kocher Maneuver to Mobilize Duodenum
- Make an Extended “U-Shaped” Incision Through the Pylorus
- Start on Stomach 6-7 cm Proximal to Pylorus
- End on Duodenum 6-7 cm Distal to Pylorus
- Closed Side-to-Side
- Start at the Middle/Pylorus
- Suture Inferior Leaf of the Stomach to the Inferior Leaf of the Duodenum
- Continue to Suture the Superior Leaf of the Stomach to the Superior Leaf of the Duodenum
- Finish with a Layer of Lembert Sutures to Invert
Jaboulay Pyloroplasty
- Used if Significant Scarring or Deformed Pylorus/Duodenal Bulb Prohibiting Other Methods
- Does Not Transect the Pylorus
- Procedure:
- Kocher Maneuver to Mobilize Duodenum
- Approximate the Duodenum Side-to-Side onto the Stomach
- Start with Posterior Lembert Sutures to Hold
- Make Two Separate Incisions Through the Antrum and then Approximated Duodenum
- Close the Inner Layer Starting with the Posterior Layer and then Extending to the Anterior Layer
- Finish with Anterior Lembert Sutures
References
- Rabben HL, Zhao CM, Hayakawa Y, Wang TC, Chen D. Vagotomy and Gastric Tumorigenesis. Curr Neuropharmacol. 2016;14(8):967-972.(License: CC BY-NC-4.0)