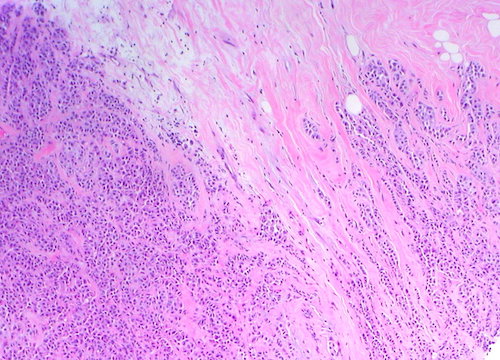
ILC: Small Cells Infiltrate Stroma & Adipose Tissue in a Single-File Pattern
Grow in Linear Plane & Infiltrate Between Tissue Planes Rather Than Distorting
Cells are Negative for E-Cadherin (Epithelial)
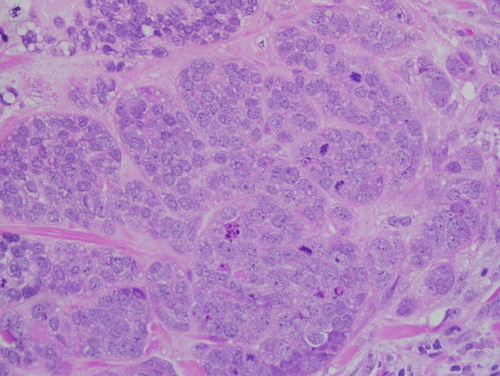
IDC: Cords & Nests of Tumor Cells with Varying Gland Formation & Fibrotic Response
Cells are Positive for E-Cadherin
Difficult to Detect on Frozen Section (Cells Similar to Lymphocytes)
Invasive Lobular Carcinoma 1
Invasive Ductal Carcinoma 2
TNM Staging
TNM
T
N
M
0
No Evidence of Primary (is – In Situ)
None
None
1
< 2 cm T1mi: ≤ 1 mm T1a: > 1 mm
T1b: > 5 mm
T1c: > 10 mm
N1mi: Micrometastases (About 200 Cells, 0.2-2.0 mm)
N1a: 1-3 Axillary Lymph Node Metastaseswith At Least One ≥ 2.0 mm
N1b: Mets in Ipsilateral Internal Mammary Sentinel Nodes
N1c: Both N1a & N1b
Distant Mets
2
> 2 cm
N2a: 4-9 Axillary Lymph Node Metastaseswith At Least One ≥ 2.0 mm
N2b: Positive Internal Mammary Nodes by Imaging with Pathologically Negative Axillary Nodes
3
> 5 cm
N3a: ≥ 10 Axillary Lymph Node Metastases or Infraclavicular Lymph Node Metastases
N3b: N1a or N2a with cN2b (Positive Internal Mammary Nodes by Imaging); or N2a with N1b
N3c: Mets in Ipsilateral Supraclavicular Lymph Nodes
4
T4a: Extension into Chest Wall (Not Muscle)
T4b: Skin Ulceration or Edema (Peau d’Orange)
T4c: Both T4a & T4b
T4d: Inflammatory Carcinoma
*Invasion of Dermis Alone Does Not Qualify as T4
Stage
T
N
M
I
A
T1
N0
M0
B
T0-1
N1mi
M0
II
A
T0-1
N1
M0
T2
N0
M0
B
T2
N1
M0
T3
N0
M0
III
A
T0-2
N2
M0
T3
N1-2
M0
B
T4
N0-2
M0
C
Any T
N3
M0
IV
Any T
Any N
M1
Treatment
Primary Treatment: Breast-Conserving Therapy (BCT) or Mastectomy
Margin: Negative Margin (“No Ink on Tumor”)
Positive Margin: Re-Excise the Margin
If Unsure Which Margin is Positive: Re-Excise All 6 Margins
Lymph Node Management:
Both Options Require Sentinel Lymph Node Biopsy (SLNB)