
Superficial Thickness 1

Superficial Partial Thickness 2

Deep Partial Thickness 3

Full Thickness

Healing from the Hair Follicles
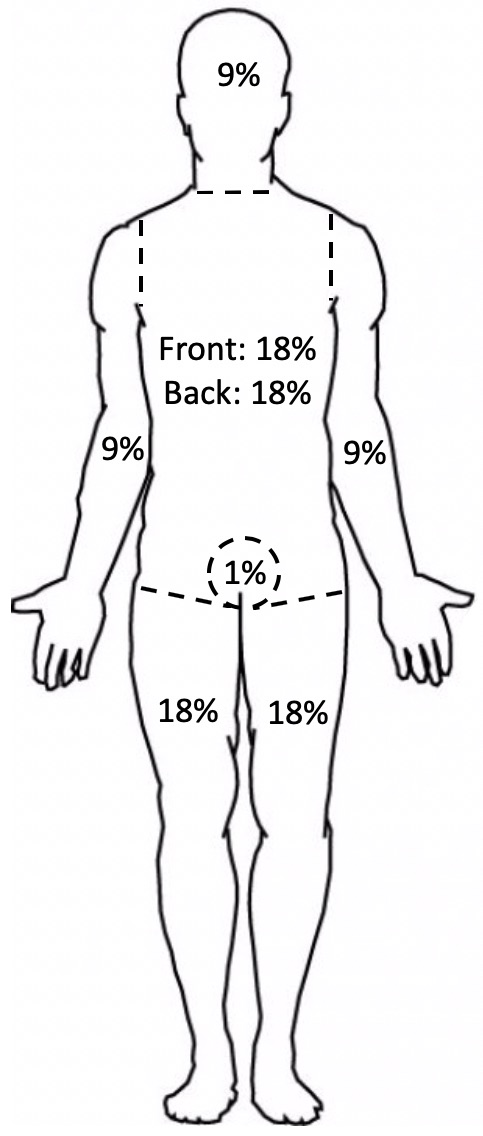
BSA Rule of 9’s

Vertical Arm Escharotomy 4
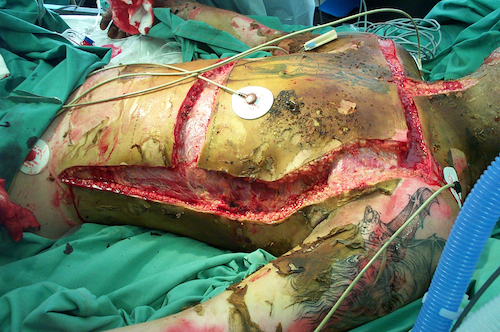
Torso “Roman Breastplate” Escharotomy 5
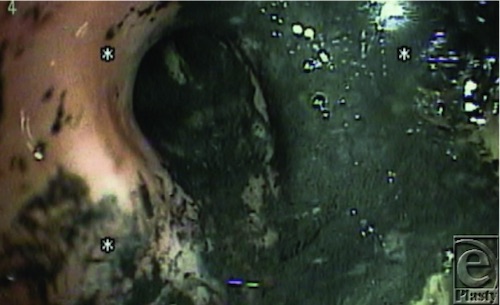
Soot in Airway 6
Superficial Thickness 1
Superficial Partial Thickness 2
Deep Partial Thickness 3
Full Thickness
Healing from the Hair Follicles
BSA Rule of 9’s
Vertical Arm Escharotomy 4
Torso “Roman Breastplate” Escharotomy 5
Soot in Airway 6