Total Gastrectomy & D2 Lymphadenectomy
- First Divide Hepatoduodenal Ligament to Visualize the Right Crus
- Divide Gastrocolic Ligament & Short Gastric Vessels
- Include Greater Curvature Lymph Nodes (Station 4) in Specimen
- Retract Stomach Up & Divide the Left Gastric Artery
- Preform a D2 Lymphadenectomy
- Start from the Proximal Common Hepatic (Station 8) & Continue to the Left Gastric Pedicle (Station 7)
- Continue Posteriorly to Celiac Node (Station 9) & Along the Splenic Artery (Station 11)
- Consider Inclusion of Splenic Hilum (Station 10) with Splenectomy
- Return Stomach to Natural Position
- Continue Dissection from Common Hepatic to the Anterior Hepatoduodenal Ligament to Include Hepatic Artery Nodes (Station 12a)
- Divide the Lesser Omentum Along the Lesser Curvature
- Include Lesser Curvature Lymph Nodes (Station 3) in Specimen
- Extend Hiatal Dissection from Right Crus to the Left Crus both Anteriorly & Posteriorly
- Include Pericardial Lymph Nodes (Stations 1-2) in Specimen
- Dissect the Proximal Duodenum to Include Pyloric Lymph Nodes (Stations 5-6)
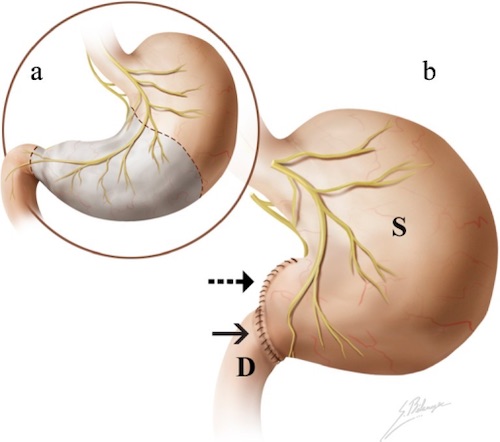
- Resection
- Transect Duodenum 1-2 cm Distal to Pylorus
- Transect the Distal Esophagus
- Send Both Margins for Frozen Section
- Proceed with Greater Omentectomy
- Reconstruction of Choice Once Frozen Section Found Negative
Total Gastrectomy Reconstructions
- Roux-en-Y Esophagojejunostomy
- Classic Roux-en-Y with a Straight Jejunal Roux Limb
- Roux-en-Y with Jejunal J-Pouch (Hunt-Lawrence)
- Procedure:
- Jejunum is Divided 20-40 cm Distal to the Ligament of Treitz
- Distal End is Folded onto Itself and Formed into a Jejunal J-Pouch of 10 cm
- Jejunojejunostomy is Made with Proximal End Set 40-50 cm Down the Distal End
- Esophagojejunostomy is Made Anvil Circular Stapler from Esophagus to the J-Pouch
- Pouch Allows Prolonged Retention of Food
- Outcomes
- Best Outcomes
- Best Nutrition & Weight Gain
- Better Quality of Life
- Lower Risk of Esophagitis, Heartburn & Dumping Syndromes
- Roux-en-Y with Looped Esophagojejunostomy
- End Esophagus to Side of Jejunum with a Small Blind End
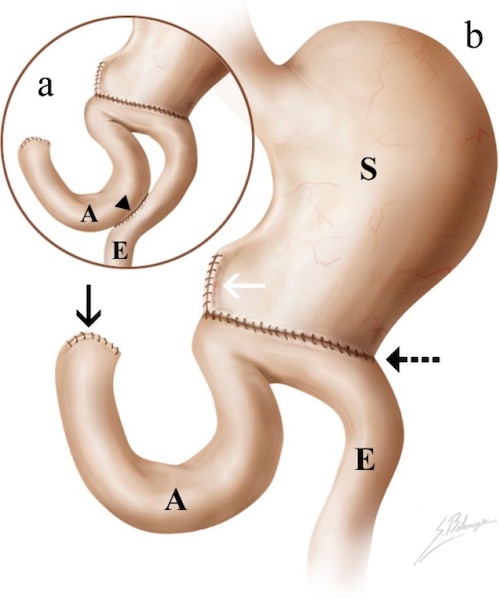
- Jejunal Interposition
- Segment of Jejunum Resected and Interposed Between Esophagus & Proximal Duodenum
- Colon Interposition
- Segment of Colon Resected and Interposed Between Esophagus & Proximal Duodenum
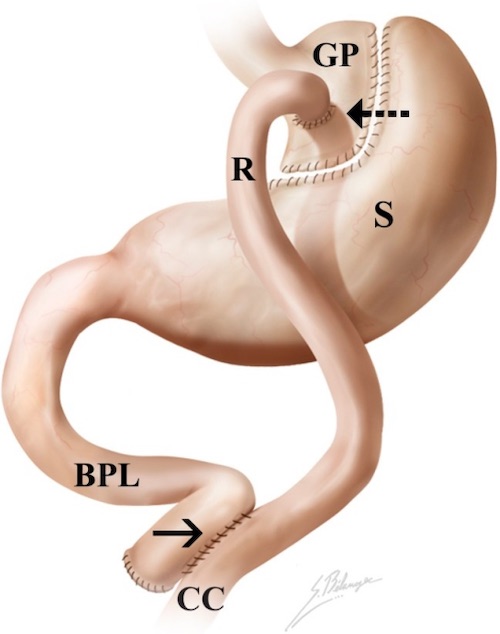
- Double Tract
- Jejunum Transected & Distal Limb is Anastomosed to the Esophagus Similar to Roux-en-Y
- The Distal End of the Proximal Limb is Anastomosed About 40-50 cm Down the Roux Limb
- The Proximal End of the Proximal Limb is Anastomosed About 15-30 cm Down the Roux Limb Creating a Second Tract