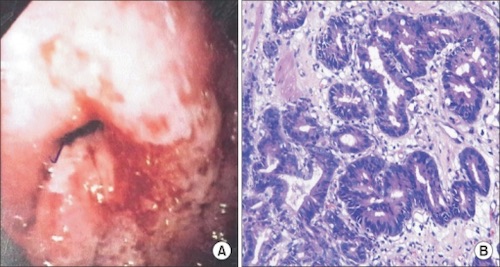
Endoscopic Mucosal Resection
- Requirements:
- ≤ 2.0 cm without Ulceration
- Well-Moderate Differentiation
- T1
- No Vascular or Lymphatic Invasion
- If Margins Positive: Surgical Resection
- May Consider Repeat Endoscopic Resection if Only the Lateral Margins are Positive
Surgical Resection
- Start with Diagnostic Laparoscopy to Evaluate Resectability
- Unresectable:
- Periaortic or Mediastinal LN
- Distant Metastases
- Peritoneal Involvement
- Invasion of Vascular Structures (Not Splenic)
- Resection:
- Approach:
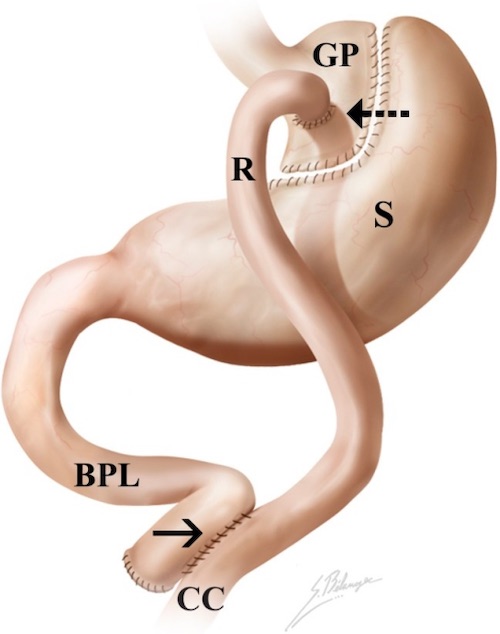
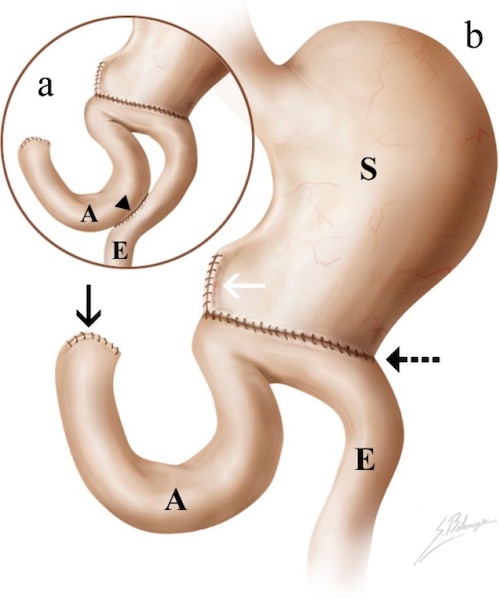
- Proximal Tumor: Total Gastrectomy
- Reconstruction: Roux-en-Y
- *Proximal Gastrectomy with Pyloroplasty Has High Risk of Alkaline Reflux Esophagitis
- Distal Tumor: Distal Gastrectomy
- Reconstruction: Roux-en-Y or Billroth II (Avoids Outlet Obstruction if Recurs)
- Margins: 4-6 cm
- Residual Disease Mn
- R0 – No Residual Disease
- R1 – Microscopic Residual Disease
- R2 – Gross Residual Disease
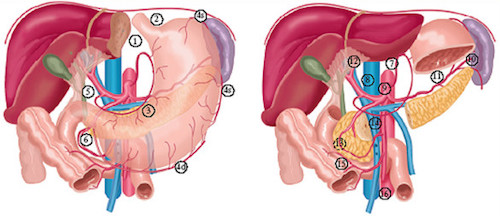
- Lymphadenectomy:
- Extent: Mn
- D1 – Perigastric Nodes (Stations 1-6)
- D2 – Celiac Axis (Stations 1-11)
- Possible Include 12a
- Generally Recommended (Debated)
- D3 – Celiac & Para-Aortic (Stations 1-16)
- LN Requirements: ≥ 15 LN for Accurate Staging
Chemotherapy
- Best Regimen Not Established
- Indications:
- Neoadjuvant: ≥ T2 or N1
- Adjuvant: ≥ T3 or N1
Palliative Treatment
- Pain: Multimodal Analgesia & Consider XRT
- Obstruction:
- Proximal: Stent
- Distal: Venting Gastrostomy, Gastrojejunostomy or Gastrectomy
- Bleeding: Endoscopy, Angioembolization or XRT