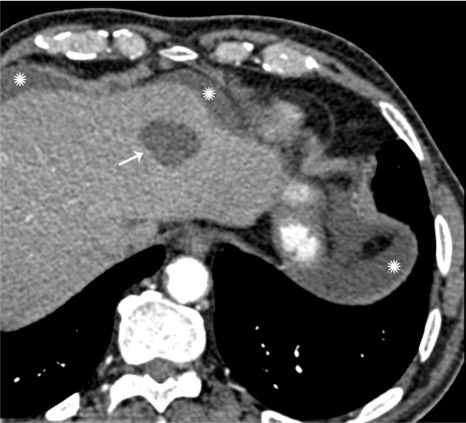
Simple Cyst of the Liver 1
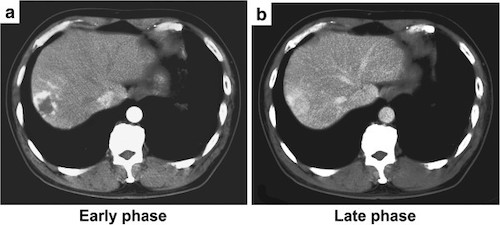
Hepatic Hemangioma. (a) Early Arterial Peripheral Enhancement, (b) Late Homogenous Attenuation 2
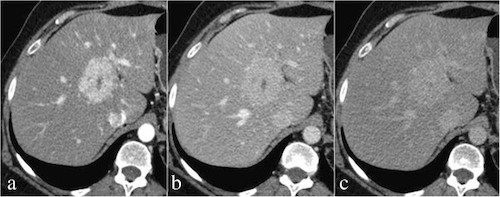
FNH. (a) Early Arterial Homogenous Enhancement with Central Scar, (b) Portal Venous Washout, (c) Delayed Phase Isodensity 3
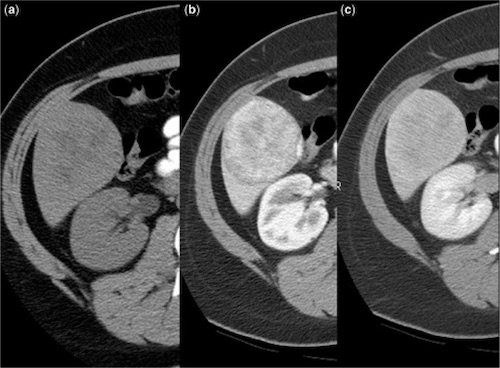
Hepatic Adenoma. (a) Precontrast, (b) Enhancement on Arterial Phase, (c) Gradual Washout on Delayed Phase 4
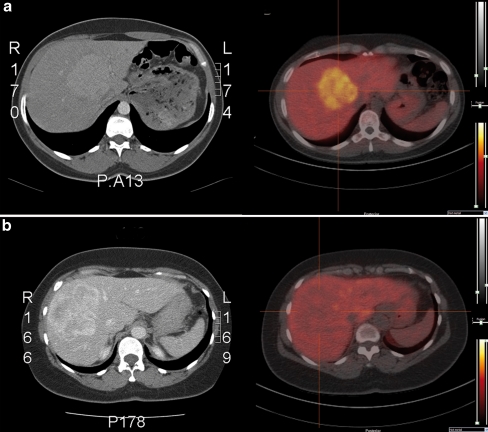
Liver Scan. (a) FNH (Hot), (b) HCA (Cold) 5