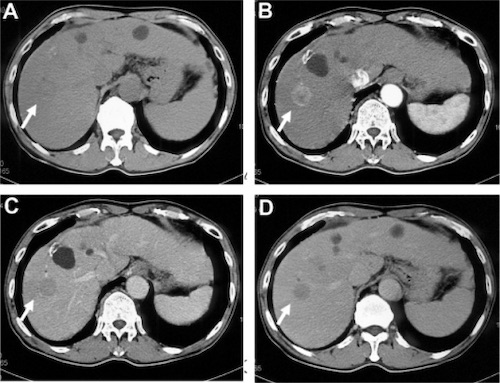
Hepatocellular Carcinoma. (a) Noncontrast, (b) Arterial Phase Enhancement, (c) Portal Phase Washout, (d) Delayed Phase Hypoattenuation 1

Liver Metastasis from Colon Cancer 2
Hepatocellular Carcinoma. (a) Noncontrast, (b) Arterial Phase Enhancement, (c) Portal Phase Washout, (d) Delayed Phase Hypoattenuation 1
Liver Metastasis from Colon Cancer 2