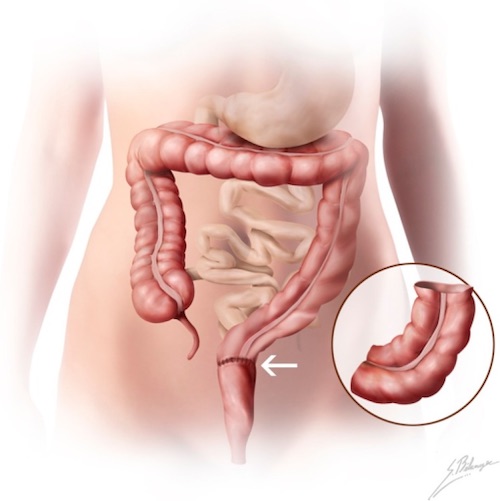
If Stage II/III – Attempt Preserve Sphincter Function
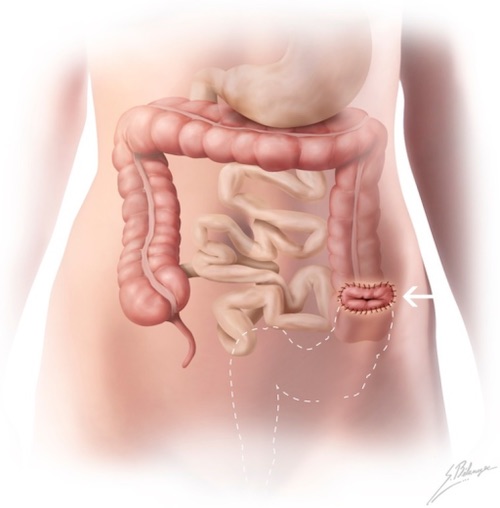
If Stage IV – Attempt for APR Instead of Only Colostomy
Adjuvant Therapy
Adjuvant Chemo:
Chemo Regimens: 5-FU, FOLFOX or CAPEOX
Indications:
T3 if Threatened Circumferential Resection Margin
T4
N+
Adjuvant XRT: Never Indicated
LAR 4
APR 4
References
Tsukada T, Nakano T, Matoba M, Sasaki S, Higashi K. False-Positive Mediastinal Lymphadenopathy on 18F-Fluorodeoxyglucose Positron Emission Tomography and Computed Tomography after Rectal Cancer Resection: A Case Report of Thoracoscopic Surgery in the Prone Position. Case Rep Oncol. 2011 Sep;4(3):569-75. (License: CC BY-NC-ND-3.0)
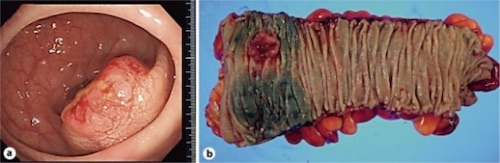
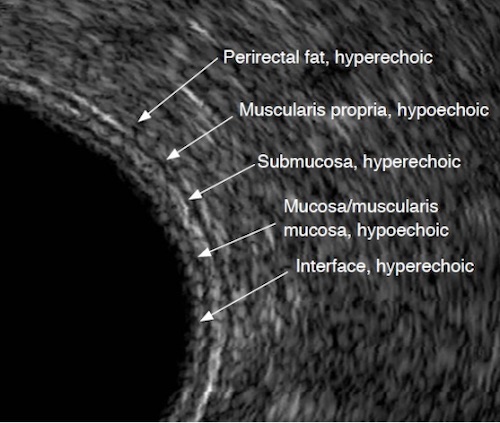
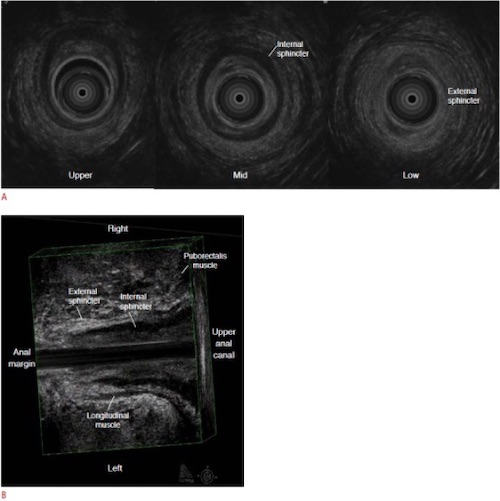
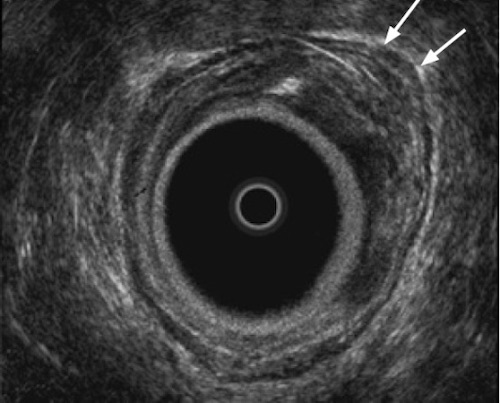
Kim MJ. Transrectal ultrasonography of anorectal diseases: advantages and disadvantages. Ultrasonography. 2015 Jan;34(1):19-31. (License: CC BY-NC-3.0)
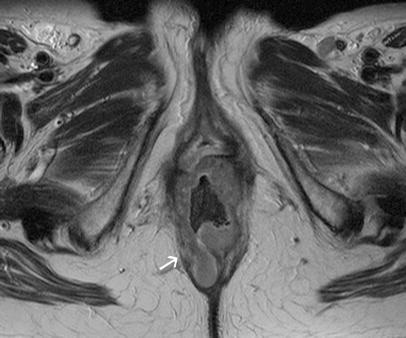
Klessen C, Rogalla P, Taupitz M. Local staging of rectal cancer: the current role of MRI. Eur Radiol. 2007 Feb;17(2):379-89. (License: CC BY-NC-2.0)
Terrone DG, Lepanto L, Billiard JS, Olivié D, Murphy-Lavallée J, Vandenbroucke F, Tang A. A primer to common major gastrointestinal post-surgical anatomy on CT-a pictorial review. Insights Imaging. 2011 Dec;2(6):631-638. (License: CC BY-2.0)