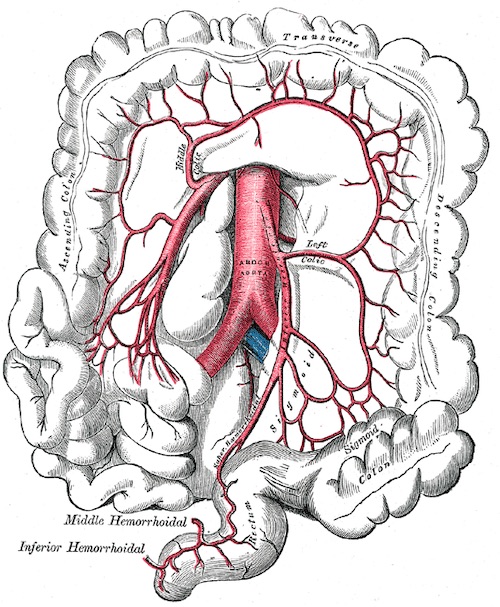
IMA Ligation
- High Ligation: Ligate Proximally, Losing the Left Colic Artery
- Colostomy Perfusion Per: Marginal Artery (Middle Colic)
- Preferred if Suspicion of Malignancy
- Low Ligation: Ligate Distally, Sparing the Left Colic Artery
- Lower Leak Risk, Otherwise Similar
- Preferred if No Suspicion of Malignancy
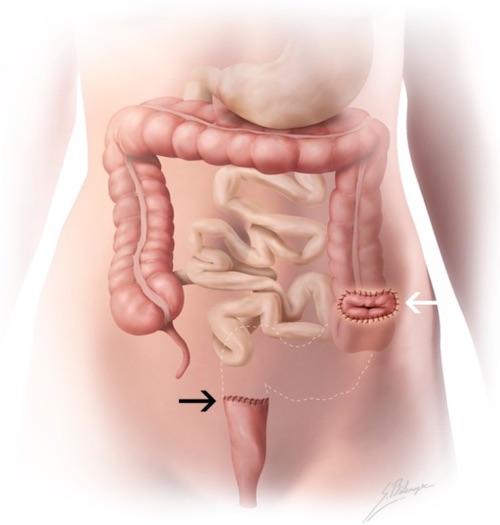
Rectosigmoid Junction Landmarks
- Where Taenia Coli Splay or Coalesce – Best Indicator
- Sacral Promontory
- Peritoneal Reflection
- Distance from Anal Verge