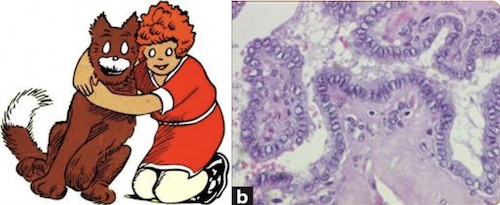
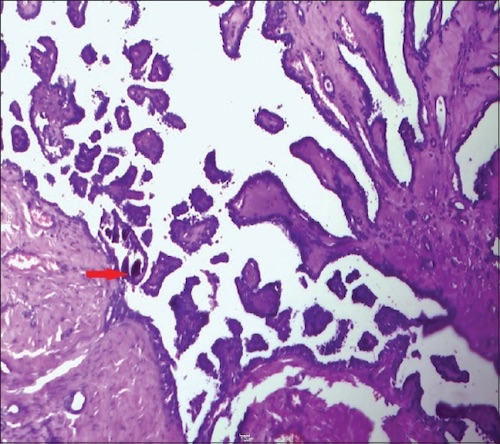
Differentiated (PTC/FTC) Thyroid Carcinoma
- Primary Surgery:
- ≥ 4 cm or Extrathyroidal Invasion: Total Thyroidectomy
- < 4 cm: Lobectomy vs. Total Thyroidectomy
- Lobectomy Generally Preferred if Small (< 1 cm)
- May Also Consider Serial Monitoring for Small (< 1 cm) PTC without Evidence of Invasive/Metastatic Features for Select Cases
- Benefits of Total Thyroidectomy:
- Removal of Potentially Multifocal Disease (Common in PTC)
- Indication for Adjuvant RAI May Not Be Fully Known Until After Surgery
- Able to Use Thyroglobulin for Postoperative Surveillance
- Indications for Total Thyroidectomy:
- Adjuvant RAI Indicated (Residual Thyroid Tissue Would Interfere with RAI)
- Contralateral Disease
- Contralateral Benign Nodularity
- Concomitant Graves’ Disease or Hypothyroidism
- History of Significant Radiation
- Family History of Significant Thyroid Cancer
- Comorbidities That Would Preclude Future Completion Thyroidectomy
- Patient Preference
- Node Management:
- ≥ 4 cm, Extrathyroidal Invasion or Central Node Mets: Central Neck Dissection
- Lateral Node Mets: Ipsilateral Lateral & Central Neck Dissections
- If Lateral Lymph Nodes are Involved the Ipsilateral Central Lymph Nodes Usually are as Well
- Adjuvant Radioactive Iodine (RAI/131I):
- Indications:
- > 4 cm
- Extrathyroidal Invasion (Local/Lymphovascular Invasion, Cervical LN or Distant Mets)
- Aggressive Histologic Findings
- Administer 4-6 Weeks After Surgery (When TSH Highest)
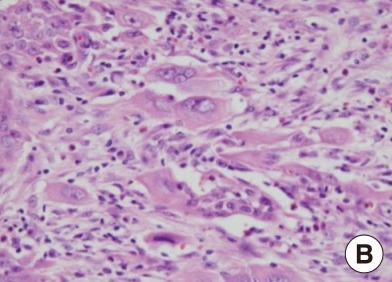
Anaplastic (Undifferentiated) Thyroid Carcinoma
- Primary Treatment: Total Thyroidectomy (If Able)
- Requirements: No Local Invasion or Metastatic Disease
- May Consider Lobectomy if There is No Evidence of Contralateral Nodularity (There is However Risk for Concomitant Foci of PTC)
- Refractory to Radioactive Iodine (RAI)
- Palliative Management:
- Consider Thyroidectomy Only for Locally Invasive Disease with Impending Airway Compromise
- Often Also Requires Placement of a Tracheostomy Tube
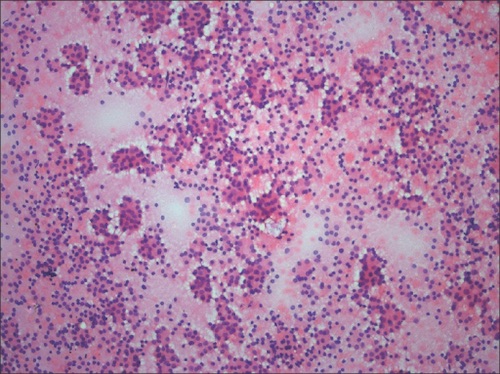
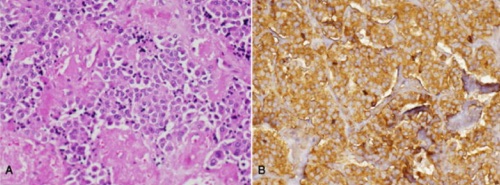
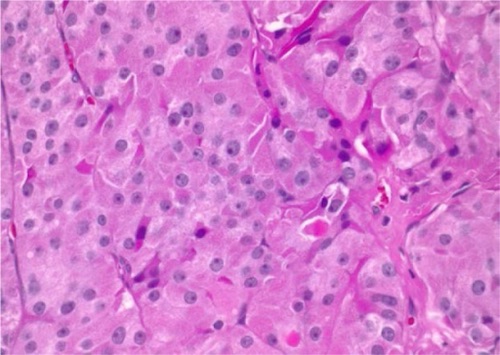
Hürthle Cell Carcinoma
- If Hürthle Cells Seen on FNA: Thyroid Lobectomy First to Diagnose
- If Diagnosed by Lobectomy or Evidence of Invasive Disease: Total Thyroidectomy
- Modified Radical Neck Dissection Required for any Clinically Evident Lymph Node Involvement
Medullary Thyroid Carcinoma
- Primary Treatment: Total Thyroidectomy & Node Dissection
- Node Dissection:
- No Lateral Neck Disease: Central Neck Dissection
- Lateral Neck Disease: Central & Lateral Neck Dissections
- Refractory to Radioactive Iodine (RAI)
- Prophylactic Thyroidectomy in MEN II:
Monitor Recurrence
- DTC (PTC/FTC): Thyroglobulin
- Best After Total Thyroidectomy
- MTC: Calcitonin & CEA