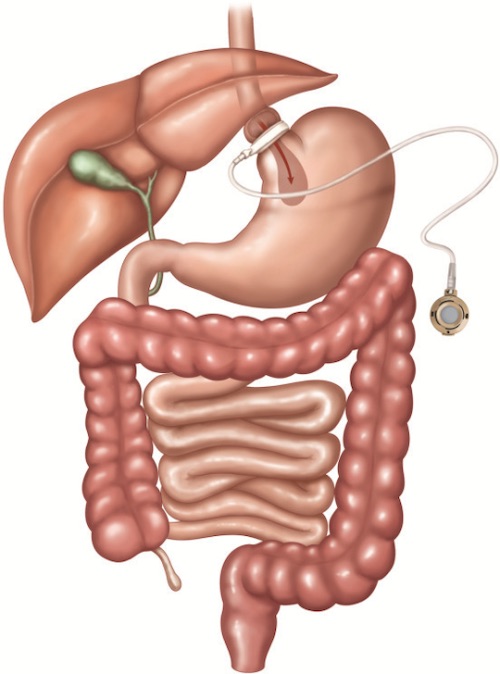
LAGB 1
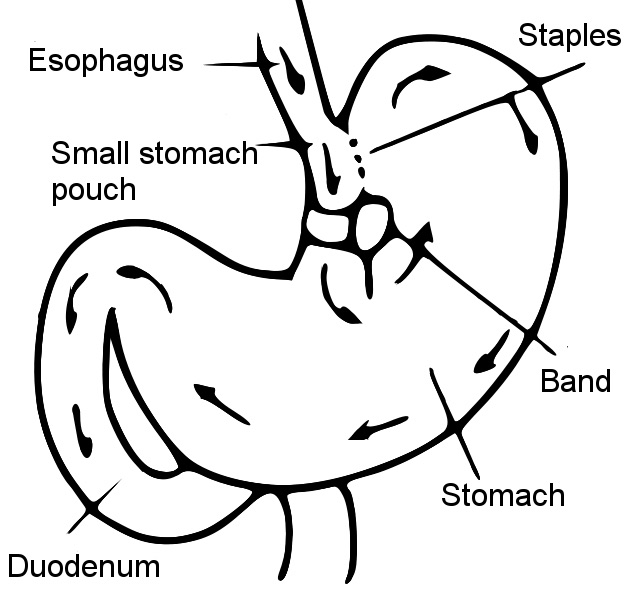
VBG 2
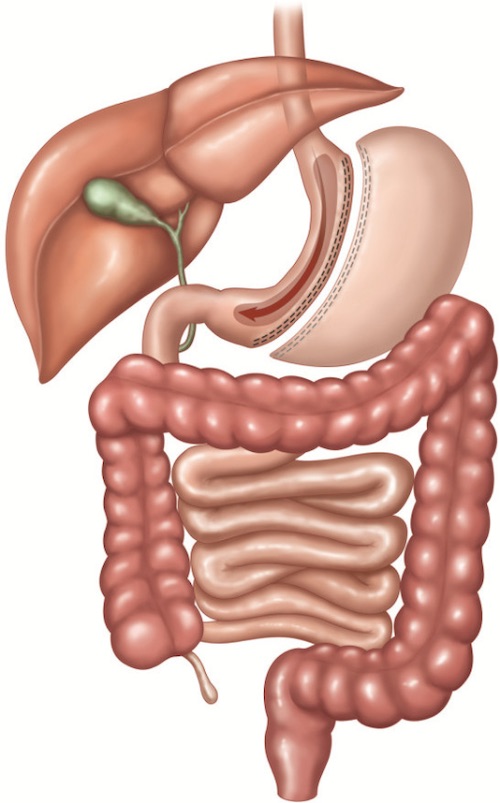
LVSG 1
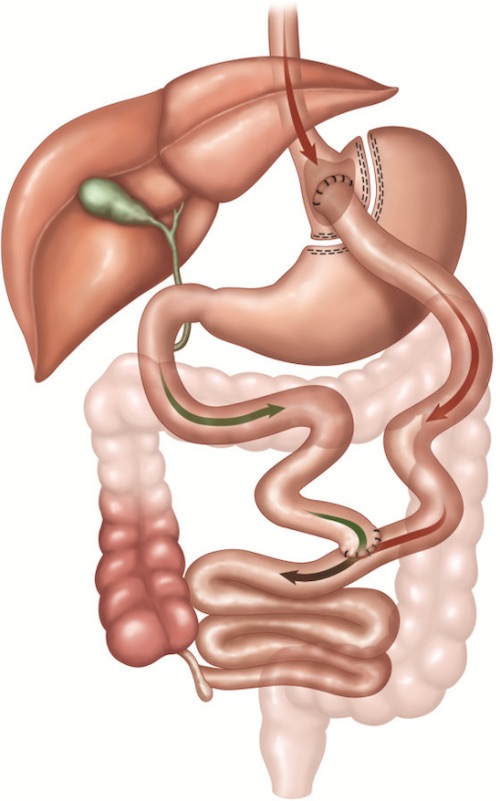
RYGB 1
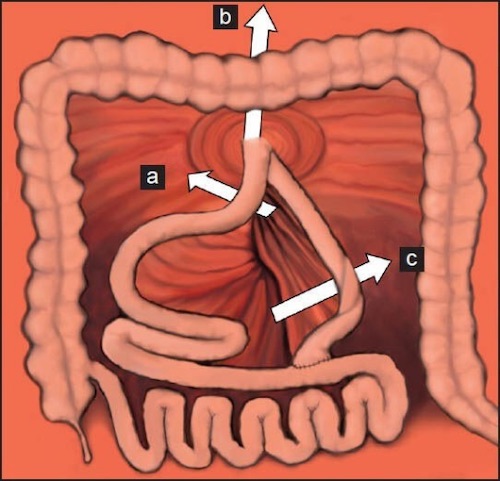
Mesenteric Defects; (a) Petersen’s Space, (b) Transverse Mesocolon Defect, (c) Jejuno-Jejunostomy Defect 3
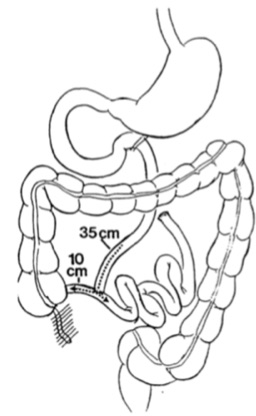
Jejunoileal Bypass 4
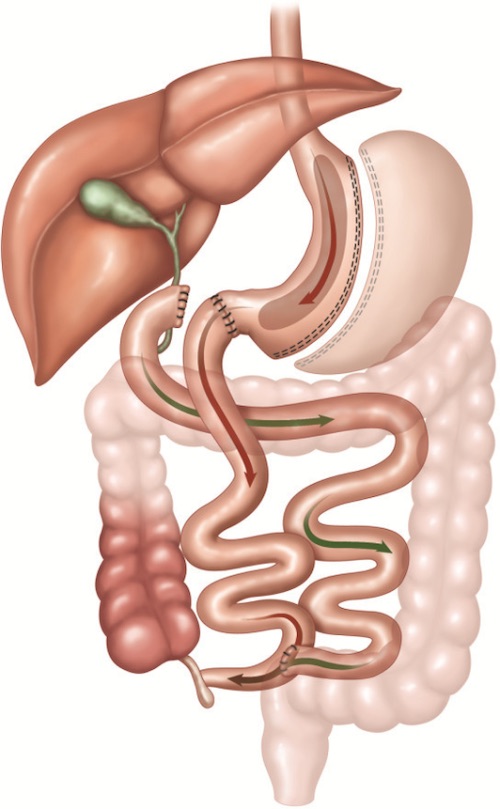
BPD-DS 1
LAGB 1
VBG 2
LVSG 1
RYGB 1
Mesenteric Defects; (a) Petersen’s Space, (b) Transverse Mesocolon Defect, (c) Jejuno-Jejunostomy Defect 3
Jejunoileal Bypass 4
BPD-DS 1