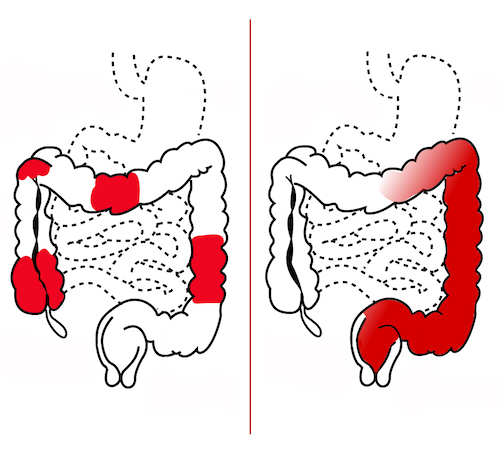
Skip Lesions of Crohn’s (Left) Compared to Continuous Lesion of UC (Right) 1

Cobblestone Mucosa of Crohn’s 2
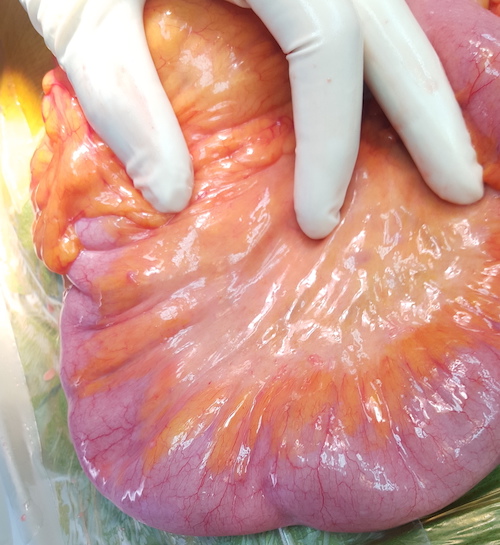
Creeping Fat of Crohn’s 3
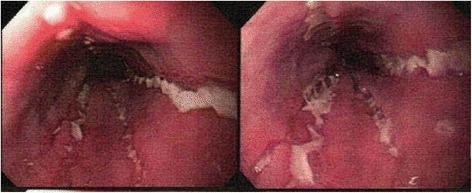
Serpiginous Ulcers of Crohn’s 4
Skip Lesions of Crohn’s (Left) Compared to Continuous Lesion of UC (Right) 1
Cobblestone Mucosa of Crohn’s 2
Creeping Fat of Crohn’s 3
Serpiginous Ulcers of Crohn’s 4