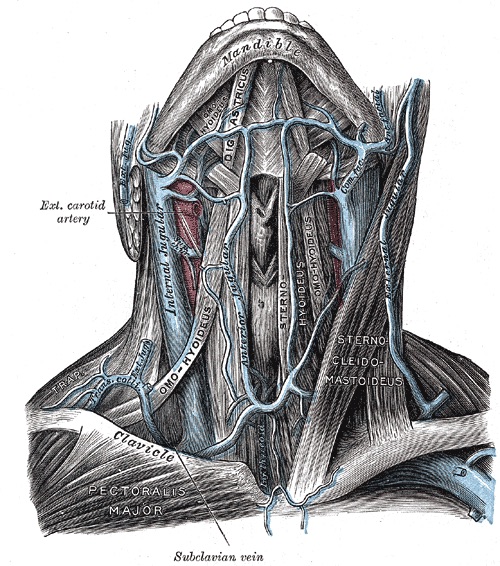
Internal Jugular Vein & Subclavian Vein 1
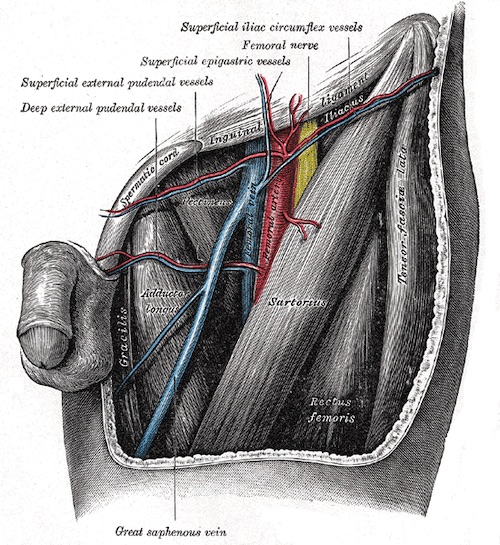
Femoral Vein 1
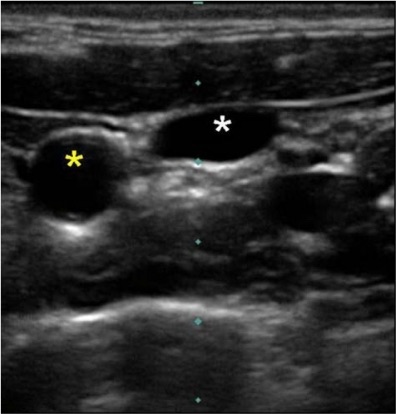
US Guidance Showing Compressibe IJ (White Star) and Noncompressible Carotid (Yellow Star) 2
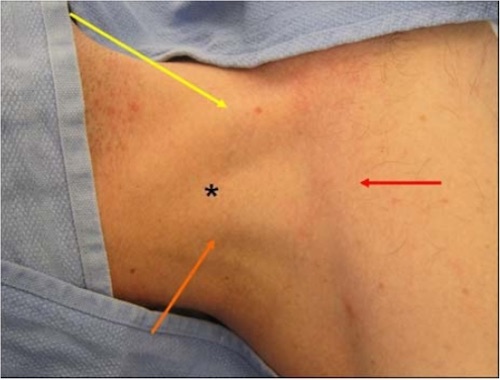
IJ Insertion (Star), SCM Sternal Head (Yellow), SCM Clavicular Head (Orange), Clavicle (Red) 2

SC Insertion (Star), Bend of Clavicle (Arrow) 2

CVC in Aorta