Immediate Relief
Initial Therapy
- Initial Tx: PPI 3-4 Weeks & Lifestyle Modifications
- 99% Effective
- If Fails: Diagnostic Testing
- Failure Defined as No Improvement After 8-12 Weeks
Diagnostic Testing
- pH Probe
- First Test to Diagnose (But Not Mandatory)
- DeMeester Score
- Components:
- Percent Total Time pH < 4
- Percent Upright Time pH < 4
- Percent Supine Time pH < 4
- Number of Reflux Episodes Total
- Number of Reflux Episode > 5 min
- Longest Reflux Episode
- Score > 14.72 Indicates Reflux
- Upper Endoscopy
- Not Required for GERD Diagnosis
- Evaluates Hiatal Hernia, Strictures, Esophagitis, Metaplasia & Malignancy
- Manometry
- To Rule Out Underlying Motility Disorder
- Indications:
- If Upper Endoscopy Normal
- Required If Planning Surgery
Antireflux Surgery
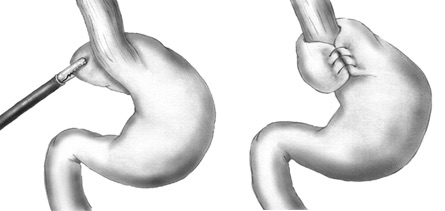
- Primary Surgery: Fundoplication
- *See Esophagus: Fundoplication
- Concurrent Dysmotility Requires Partial Fundoplication
- May Consider Roux-en-Y Gastric Bypass if Morbidly Obese with Indications for Bariatric Surgery – Small Pouch is Created with Minimal Acid Production
- Indications:
- Failed Medical Management
- GERD Complications (Esophagitis or Stricture)
- PPI Side Effects (Headache, Nausea, Vomiting or Diarrhea)
- Patient Preference
- Poor Compliance
- Contraindications:
- Unable to Tolerate Surgery
- High-Grade Dysplasia or Carcinoma
- Morbid Obesity – Relative Contraindication
- Best Predictors of Success:
- Typical Symptoms
- Typical Symptoms Resolve in 90% of Patients
- Atypical Symptoms Resolve in 60-70% of Patients
- Symptoms Improved on PPI
- High Esophageal pH
Other Modern Antireflux Procedures
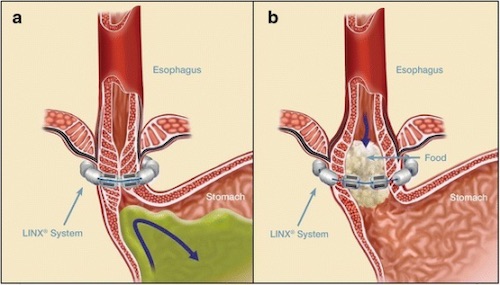
- Magnetic Sphincter Augmentation (LINX Device)
- Ring Made of Magnets Placed Around the LES
- Increases LES Pressure while Closed
- Can Open with Pressure while Swallowing to Permit Food Passage
- Exact Indications Poorly Defined
- Benefits Over Fundoplication:
- Shorter Surgery & Faster Recovery
- Easily Reversible
- Does Not Permanently Alter Stomach Anatomy
- Retains Ability to Belch/Vomit
- Potential Risk for Esophageal Erosion (0.3%)
- Should Eat Frequent Solid Meals Postop to Prevent Scarring Capsule Formation & Resulting Dysphagia
- Stretta Procedure
- Endoscopic Controlled Radiofrequency Energy Applied to the LES
- Induces Inflammation, Collagen Deposition & Muscular Thickening
- Transoral Incisionless Fundoplication (TIF)
- Endoscopic Full Thickness Plication
- Partial Fundoplication (200-300-Degrees)